Physical Exercise and Cognitive Function in Post-stroke Patients: A Systematic Review with Meta-Analysis
Arturo Gallego Hernández
Noelia González-Gálvez
*Corresponding author: Noelia González-Gálvez ngonzalez@ucam.edu
Cite this article
Gallego Hernández, A. & González-Gálvez, N. (2021). Physical Exercise and Cognitive Function in Post-stroke Patients: A Systematic Review with Meta-Analysis. Apunts Educación Física y Deportes, 146, 1-10. https://doi.org/10.5672/apunts.2014-0983.es.(2021/4).146.01
Abstract
Up to 80% of stroke survivors have cognitive dysfunction, which affects motor function and quality of life. There is a need to understand which physical activity prescription is most recommendable for cognitive function and to determine the effect of physical exercise programmes on cognitive function in post-stroke patients by identifying the best frequency, length and type of programme. The PRISMA guidelines were followed and the methodology was registered in PROSPERO (number CRD42020183529). The studies chosen were randomised controlled trials. The search was conducted in four databases, namely PubMed, Cochrane, SPORTDiscus and WOS, and concluded on 12 June 2020. Methodological quality was assessed using the PEDro scale score. The meta-analysis reveals that the experimental group had greater gains in cognitive function than the control group (SMD = 2.26; p .001). It shows that there is a greater effect on cognitive function in studies which include an adult population versus those that include an older adult population (SMD = 1.82; p = .014). Strength training provides a significantly greater gain than aerobic training (SMD= –1.88; 95% CI –3.7, –0.1; p = .040). A physical exercise programme significantly improves cognitive function in post-stroke patients and may have a greater effect than rehabilitation programmes. The programme should last at least six weeks, with a frequency of three sessions per week and a per-session length of at least 30 minutes.
Introduction
Stroke is one of the leading causes of disability and death worldwide (Go et al., 2014). Specifically, more than 14 million people suffer a stroke each year, and around 10% of them die (Carnesoltas et al., 2013). Suffering a stroke has a negative impact on the subsequent quality of life of those who manage to survive it, since it affects all areas of the individual: physical health and psychological state are reduced, autonomy and independence are diminished and cognitive function (executive, attention and memory) is significantly impaired (Mesa et al., 2016). Up to 80% of stroke survivors experience cognitive dysfunction, directly influencing motor function and quality of life (Sun et al., 2014), and stroke is the second leading cause of dementia worldwide (Alvarez, 2008). Although post-stroke patients may recover from the ensuing physical after-effects, cognitive impairments may restrict autonomy and independence (Gottesman & Hillis, 2010; Wagle et al., 2011). Identifying effective treatments to improve cognitive function is therefore of paramount importance (Debreceni-Nagy et al., 2019), and a multidisciplinary rehabilitation approach is needed to improve levels of motor and functional disability (Go et al., 2014).
Physical inactivity is a known predictor of stroke, as a sedentary lifestyle is associated with a higher probability of having one (Martínez-Vila & Irimia, 2000). Similarly, exercise can improve quality of life in the general population (Solà-Serrabou et al., 2019) and also be of benefit to the cardiovascular system (Betrán Piracés et al., 2003) and cognitive function in individuals after suffering a stroke in both executive functions and memory (Freudenberger et al., 2016; Vanderbeken & Kerckhofs, 2016; Yeh et al., 2019).
Some authors have conducted systematic reviews to synthesise the research on the effect of physical exercise on cognitive function in people who have had a stroke (Cumming et al., 2012; Oberlin et al., 2017). However, these studies include intervention programmes which combine physiotherapy and physical exercise and do not report which frequency, length or type of exercise has the greatest benefits for cognitive function in post-stroke patients. Therefore, the objectives of this systematic review with meta-analysis were: a) to determine the effect of physical exercise on cognitive function in post-stroke patients, and b) to synthesise the original studies on the effect of physical exercise programmes on cognitive function in post-stroke patients to identify the best frequency, length and type of programme.
Methodology
Study design
The studies included in this systematic review and meta-analysis examine the effect of various physical exercise programmes on cognitive function in post-stroke patients. The studies chosen were randomised controlled trials (RCTs). The search strategy, together with the inclusion criteria and additional information, was registered beforehand in the PROSPERO international database of prospectively registered systematic reviews (number CRD42020183529). This systematic review with meta-analysis follows the principles set out in the PRISMA (Preferred Reporting Items for Systematic Reviews) guidelines (Liberati et al., 2009; Moher et al., 2015).
Inclusion criteria
The inclusion criteria were: a) articles published in indexed journals, b) articles published in English, Spanish and Portuguese only, c) articles involving patients who had previously suffered a stroke, d) RCTs, and e) studies implementing a physical exercise programme. The exclusion criteria were: a) studies in progress, b) studies involving people with amputation/limitation of any limb that contraindicates walking/exercise, c) studies published as abstracts, notes or letters to the editor or short publications, d) studies published at conferences, and e) studies implementing physiotherapy programmes, manipulation and/or breathing techniques in conjunction with physical exercise.
Search strategies
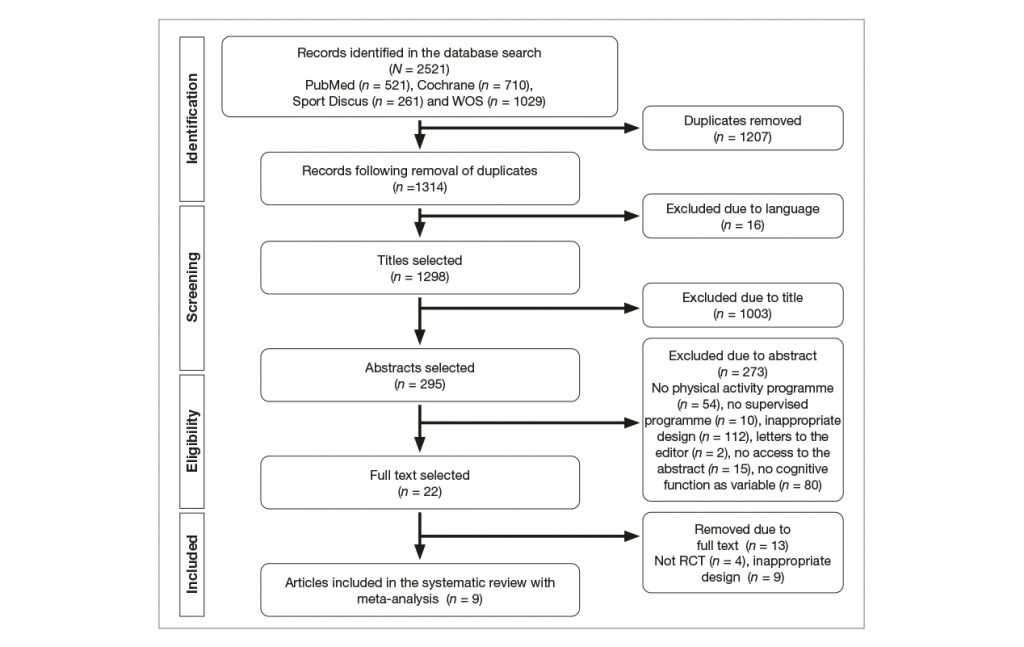
The following search engines were used to search for information: PubMed, Cochrane, Sport Discus and WOS. The search strategy was based on the use of keywords and Boolean operators, including: stroke AND physical activity, stroke AND sport, stroke AND strength training, stroke AND endurance training, stroke AND resistance training, stroke AND physical therapy, stroke AND aerobic training, stroke AND endurance exercise, stroke AND aerobic exercise, stroke AND strength exercise and stroke AND resistance exercise. The search ended on 12 June 2020. The flowchart is shown in Figure 1.
Data extraction
Data extraction and quality assessment were performed by two reviewers (AGH and NGG) independently. Disagreements over information were resolved by repeating data extraction or unobserved assessment of information from previously conducted reviews. In this regard, Cohen’s Kappa index was calculated, presenting high inter-reviewer reliability (Kappa = .810) (McHugh, 2012).
Assessment of methodological quality
The Physiotherapy Evidence Database (PEDro) scale was used to assess the methodological quality of the included studies (Maher et al., 2003). Table 1 shows the PEDro scale scores for each study, assuming values of 8, which was considered acceptable.
Data analysis
The statistical analysis and meta-analysis were performed using the Comprehensive Meta-Analysis program (version 3, Englewood, USA). For the analysis of this study, the quantitative mean and standard deviation of the pre-test and post-test, as well as the sample size, were used for the control group and the experimental group. Pre-/post-test changes were calculated for analysis. When the same study included several sub-variables of cognitive function, these were included as different cases in the analysis. If the studies did not show the necessary data, these were calculated. SEs and the CIs were used to calculate SD. The DerSimonian-Laird (Cohen’s) method was used. Heterogeneity was assessed by means of Cochran’s Q test (chi2), Higgins’ I2 statistic and significance (p) to determine the most appropriate analysis: fixed or random effects (Ioannidis, 2008). DerSimonian-Laird (Cohen) was interpreted as small (0 to 0.2), moderate (0.3 to 0.7) or large (≥ 0.8) (Cohen, 1988). Egger’s test (Egger et al., 1997) and Fail Safe N (Rosenthal, 1979) were calculated to determine publication bias. A funnel plot was created. Significance was determined at p < .05.
Results
Characteristics of the studies
The article selection and search strategy employed in this systematic review with meta-analysis resulted in a total of nine articles.
The included articles were RCTs, and they featured a total of 355 participants in the experimental group and 362 in the control group. The analysed articles were published between 2001 and 2020.
The characteristics of the included studies are shown in Table 2.
Effect of physical exercise on post-stroke patients
The meta-analysis reveals that the effect of physical exercise programmes on cognitive function in post-stroke patients is significantly more beneficial than the effect of any other programme or no programme (Figure 2) (OR = 2.26; 95% CI = 1.0 to 3.5; Z = 3.63; p = < .001).
To examine whether there were differences by possible contaminating variables, subgroups were established by age, length of the intervention in weeks, frequency of sessions per week, length of sessions, type of physical exercise programme and participant age. The age variable was divided between adults (< 65 years) and older adults (≥ 65 years). To make the groups for frequency and length of the programme, the medians of the weeks of intervention, weekly frequency and session length variables were analysed, obtaining 12 weeks, three sessions per week and 60 minutes per session, respectively. The type of physical exercise variable was divided into aerobic, strength or combined training. For the purpose of comparison, changes were transformed into percentages. Table 3 shows the analysis of the effect of the physical exercise programmes included in this systematic review on cognitive function according to the aforementioned classifications. It shows that there is a greater effect on cognitive function in the studies that include the adult population versus those that include the older adult population. When the subgroup with extreme gains in the variable is removed (Ozdemir et al., 2001), the results remain significant (SMD = 1.96; 95% CI 0.4, 3.6; p = .016). A difference is observed in relation to the type of programme implemented significantly favouring strength training over aerobic training. However, this difference is no longer significant after the group presenting an extreme change in the variable is removed (Ozdemir et al., 2001).
Table 2
Characteristics of the included studies.
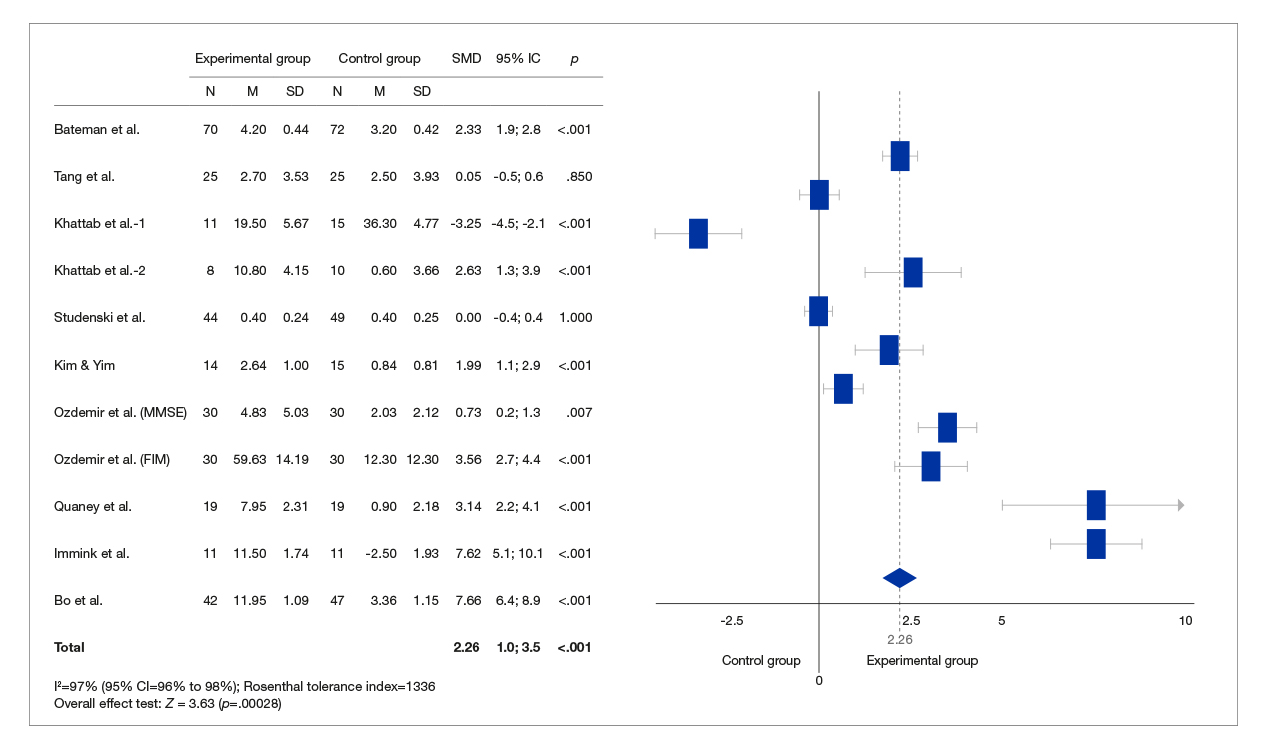
Note. N: sample size; M: mean; SD: standard deviation; SMD: standardised mean difference; 95% CI: 95% confidence interval; p: p significance value.
Table 3
Analysis of the effect of physical exercise programmes on cognitive function by length in weeks, weekly frequency, session length and type of physical exercise programme implemented.
Discussion
The first objective of this systematic review with meta-analysis was to determine the effect of physical exercise on cognitive function in post-stroke patients.
The meta-analysis revealed that physical exercise has a significant positive effect on cognitive function compared to the control group. These results are in line with other research (Cumming et al., 2012; Oberlin et al., 2017). Cumming et al. (2012) conducted a systematic review including 12 studies. Their meta-analysis of nine of the studies showed an improvement in favour of the experimental group, although it was not significant (SMD= 0.20; p = .719). Oberlin et al. (2017) performed their meta-analysis including a total of 14 RCTs. These authors also found a significant improvement (SMD = 0.304; p < .001).
It should be noted that both Cumming et al. (2012) and Oberlin et al. (2017) featured physiotherapy intervention programmes in their inclusion criteria in addition to physical exercise programmes. In this regard, this meta-analysis has a larger effect size on cognitive function than these studies. Similarly, two of the studies included in this systematic review (Kim & Yim, 2017; Studenski et al., 2005) used a physiotherapy programme in the control group. Studenski et al. (2005) show the same results after applying both programmes, while Kim and Yim (2017) obtained significantly better results in the physical exercise group. These findings suggest that a physical exercise programme can reduce the cognitive decline caused by stroke and its effect may be greater than that achieved with a physiotherapy programme.
The second objective of this systematic review with meta-analysis was to synthesise the original studies on the effect of physical exercise programmes on cognitive function in post-stroke patients by identifying the best frequency, length and type of programme.
As for the age of the participants in this research, four studies implemented their physical exercise programmes in adults (<65 years) (Bateman et al., 2001; Immink et al., 2014; Kim & Yim, 2017; Ozdemir et al., 2001) while five studies used programmes in older adults (≥65 years) (Bo et al., 2019; Khattab et al., 2020; Quaney et al., 2009; Studenski et al., 2005; Tang et al., 2016). The eexamination of whether there were differences in the effect of the physical exercise programme on cognitive function by age suggests that adults improved significantly more than older adults. This might be due to the relationship between age and cognitive decline. Cognitive decline is considered an inevitable part of ageing and can range from mild cognitive impairment to chronic neurodegenerative disease (Karantzoulis & Galvin, 2011). Programmes aimed at older post-stroke patients should probably include other aspects. A systematic review of healthy older adults showed greater improvements in cognitive function after programmes that combined physical exercise and cognitive training compared to those that featured only physical exercise (Gheysen et al., 2018). The paper by Bo et al. (2019) compared a combined training programme with a cognitive training programme and found that the combined training programme yielded greater cognitive function benefits than the cognitive training programme. Consequently, programmes that include a multi-component approach and cognitive training are recommended.
The mean length of the programmes was 13.6 weeks, with an average frequency of 3.8 sessions per week and 55.5 minutes per session. In this regard, the analysis showed that there was no difference between using a programme of more than 12 weeks or a shorter one, and that a frequency of more than three sessions per week or a longer session length does not lead to greater improvements in cognitive function. These results are in line with a recent meta-analysis on the effect of physical exercise on cognitive function in healthy older adults (Gheysen et al., 2018). The meta-analysis by Oberlin et al. (2017) indicated greater improvements in studies which conducted an intervention lasting less than three months. Our results exhibit the same tendency, although it is not significant. These findings might be due to non-compliance with the training principles used in exercise programmes targeting post-stroke patients, in particular the principle of progression. A recent systematic review showed that the training principles employed in physical exercise programmes in this population are inconsistent (Ammann et al., 2014). Accordingly, it is recommended that physical exercise programmes in post-stroke patients designed to improve cognitive function pay special attention to training principles and last at least six weeks with a frequency of three sessions per week and a per-session length of at least 30 minutes.
In relation to the type of physical exercise programme, five subgroups used aerobic exercise programmes (Bateman et al., 2001; Khattab et al., 2020; Quaney et al., 2009; Tang et al., 2016), three subgroups applied strength programmes (Immink et al., 2014; Ozdemir et al., 2001) and three employed combined programmes (Bo et al., 2019; Kim & Yim, 2017; Studenski et al., 2005). The analysis shows that sessions implementing strength exercises were more beneficial than those that included aerobic exercise work. However, this difference ceases to be significant after the group presenting an extreme change in the cognitive function variable is removed (Ozdemir et al., 2001). Similarly, the group of studies using strength programmes does not include older adults, compared to the aerobic training group, which includes four studies with older adults (Bateman et al., 2001; Khattab et al., 2020; Quaney et al., 2009; Tang et al., 2016), and the combined training group, which includes one (Studenski et al., 2005). These results are in line with those produced by the meta-analysis conducted by Oberlin et al. (2017). These authors show that aerobic-only training did not show positive results in terms of cognitive function, whereas strength training did. However, they do not indicate whether these differences between groups were significant. Thus, aerobic training increases cerebral blood volume (Pereira et al., 2007), while strength training fosters greater vascularisation and improves essential supply to the brain, meaning that they both improve cognitive function (Tsai et al., 2015). Similarly, an increase in brain-derived neurotrophic factor (BDNF) protein has been linked to exercise in the improvement of cognitive function (Winter et al., 2007). The number of RCTs needs to be increased so as to identify the type of exercise which is most recommended for improving cognitive function in stroke patients.
Practical application
This systematic review with meta-analysis shows that a physical exercise-only programme delivers significant positive results for cognitive function in post-stroke patients. However, other variables such as participant age and training principles need to be addressed in order to maximise the benefits. These results herald a new finding for doctors and physical trainers with regard to reducing cognitive decline in these patients and thus improving their quality of life. It is recommended that a physical exercise programme in post-stroke patients intended to enhance cognitive function should pay special attention to training principles, be based mainly on strength exercises and last at least six weeks with a frequency of three sessions per week and a per-session length of at least 30 minutes.
Limitations
The main limitation of this systematic review with meta-analysis is the small number of RCTs conducted to date. This aspect constrains comparisons between groups and means that the number of original RCT investigations needs to be increased. Another limitation is that all the studies do not all use the same tool to assess cognitive ability and the results had to be translated into percentages in order to draw comparisons.
Conclusions
A physical exercise programme significantly improves cognitive function in post-stroke patients and its effect may be greater than that of rehabilitation programmes.
Combined programmes of physical exercise and cognitive training will probably be needed in post-stroke older adults compared to younger and middle-aged adults due to age-related cognitive impairment.
It is recommended that a physical exercise programme in post-stroke patients with the aim of improving cognitive function pay special attention to training principles and last at least six weeks with a frequency of three sessions per week and a per-session length of at least 30 minutes.
There is moderate evidence that suggests that strength training programmes are the most beneficial in improving cognitive function in this population. However, more research is needed to indicate which type of physical exercise programme is most helpful for post-stroke patients.
References
[1] Alvarez, J. (2008). Mortalidad hospitalaria por ictus. Revista Española de Cardiología, 61(10), 1007-1009.
[2] Ammann, B. C., Knols, R. H., Baschung, P., Bie, R. A. De, & Bruin, E. D. De. (2014). Application of principles of exercise training in sub-acute and chronic stroke survivors : a systematic review. BMC Neurology, 14, 1-11. https://doi.org/10.1186/s12883-014-0167-2
[3] Bateman, A., Culpan, F. J., Pickering, A. D., Powell, J. H., Scott, O. M., & Greenwood, R. J. (2001). The effect of aerobic training on rehabilitation outcomes after recent severe brain injury: A randomized controlled evaluation. Archives of Physical Medicine and Rehabilitation, 82(2), 174-182. https://doi.org/10.1053/apmr.2001.19744
[4] Betrán Piracés, M., Casterad Más, J., & Serra Puyal, J. (2003). Efectos de un programa de actividad física sobre los parámetros cardiovasculares en una población de la tercera edad. Apunts Educación Física y Deportes, 3(73), 42–48.
[5] Bo, W., Lei, M., Tao, S., Jie, L. T., Qian, L., Lin, F. Q., & Ping, W. X. (2019). Effects of combined intervention of physical exercise and cognitive training on cognitive function in stroke survivors with vascular cognitive impairment: a randomized controlled trial. Clinical Rehabilitation, 33(1), 54-63. https://doi.org/10.1177/0269215518791007
[6] Carnesoltas, L., Serra, M., & O’Farrill, R. (2013). Factores de riesgo y mortalidad por neumonía intrahospitalaria en la Unidad de Terapia Intensiva de Ictus. Medwave, 13, 1-2.
[7] Cohen, J. (1988). Statistical power analysis for the behavioral sciences .Lawrence Earlbaum Associates (ed.); 2nd ed.
[8] Cumming, T. B., Tyedin, K., Churilov, L., Morris, M. E., & Bernhardt, J. (2012). The effect of physical activity on cognitive function after stroke: a systematic review. International Psychogeriatrics, 24(4), 557-567. https://doi.org/10.1017/S1041610211001980
[9] Debreceni-Nagy, A., Horvath, J., Bajuszne Kovacs, N., Fulop, P., & Jenei, Z. (2019). The effect of low-intensity aerobic training on cognitive functions of severely deconditioned subacute and chronic stroke patients: a randomized, controlled pilot study. International Journal of Rehabilitation Research. Internationale Zeitschrift Fur Rehabilitationsforschung. Revue Internationale de Recherches de Readaptation, 42(3), 275-279. https://doi.org/10.1097/MRR.0000000000000346
[10] Egger, M., Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test measures of funnel plot asymmetry. Thebmj, 315, 629-634.
[11] Freudenberger, P., Petrovic, K., Sen, A., Töglhofer, A., Fixa, A., Hofer, E., Perl, S., Zqwiker, R., Seshadri, S., Schimidt, R., & Schmidt, H. (2016). Ftiness and cognition in the elderly. The Austrian Stroke Prevention Study. Neurology, 86(5), 418-424.
[12] Gheysen, F., Poppe, L., Desmet, A., Swinnen, S., Cardon, G., Bourdeaudhuij, I. De, Chastin, S., & Fias, W. (2018). Physical activity to improve cognition in older adults : can physical activity programs enriched with cognitive challenges enhance the effects ? A systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity, 15(63), 1-13.
[13] Go, A. S., Mozaffarian, D., Roger, V. L., Benjamin, E. J., Berry, J. D., Blaha, M. J., Dai, S., Ford, E. S., Fox, C. S., Franco, S., Fullerton, H. J., Gillespie, C., Hailpern, S. M., Heit, J. A., Howard, V. J., Huffman, M. D., Judd, S. E., Kissela, B. M., Kittner, S. J., … Heart, A. (2014). AHA Statistical Update Executive Summary : Heart Disease and Stroke Statistics – 2014 Update A Report From the American Heart Association Writing Group Members. Circulation, 129(3), 399-410. https://doi.org/10.1161/01.cir.0000442015.53336.12
[14] Gottesman, R., & Hillis, A. (2010). Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol, 9, 895-905. https://doi.org/10.1016/S1474-4422(10)70164-2.Predictors
[15] Immink, M. A., Hillier, S., & Petkov, J. (2014). Randomized controlled trial of yoga for chronic poststroke hemiparesis: Motor function, mental health, and quality of life outcomes. Topics in Stroke Rehabilitation, 21(3), 256-271. https://doi.org/10.1310/tsr2103-256
[16] Ioannidis, J. P. A. (2008). Interpretation of tests of heterogeneity and bias in meta-analysis. Journal of Evaluation in Clinical Practice, 14(5), 951-957. https://doi.org/10.1111/j.1365-2753.2008.00986.x
[17] Karantzoulis, S., & Galvin, J. (2011). Distinguishing Alzheimer’s disease from other major forms of dementia. Expert Rev Neurother, 11(11), 1579-1591. https://doi.org/10.1586/ern.11.155.Distinguishing
[18] Khattab, S., Eng, J. J., Liu-Ambrose, T., Richardson, J., MacDermid, J., & Tang, A. (2020). Sex differences in the effects of exercise on cognition post-stroke: Secondary analysis of a randomized controlled trial. Journal of Rehabilitation Medicine, 52(1), 1-8. https://doi.org/10.2340/16501977-2615
[19] Kim, J., & Yim, J. (2017). Effects of an exercise protocol for improving handgrip strength and walking speed on cognitive function in patients with chronic stroke. Medical Science Monitor, 23(5402). https://doi.org/10.12659/MSM.904723
[20] Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., & John, P. A. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol, 62(10), 1-34. https://doi.org/10.1136/bmj.b2700
[21] Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., & Elkins, M. (2003). Reliability of the PEDro Scale for Rating Quality of Randomized. Physical Therapy, 83(8), 713-721.
[22] Martínez-Vila, E., & Irimia, P. (2000). Factores de riesgo del ictus Risk factors of the stroke. In Anales del Sistema Sanitario de Navarra, 23, 25-31.
[23] McHugh, M. L. (2012). Lessons in biostatistics interrater reliability : the kappa statistic. Biochemica Medica, 22(3), 276-282. https://hrcak.srce.hr/89395
[24] Mesa, Y., Fernández, O., Hernández, T., & Parada, Y. (2016). Calidad de vida en pacientes post-ictus : factores determinantes desde la fase aguda Quality of life in post-ictuspatients : determinants factors from the acute phase. Revista Habanera de Ciencias Médicas, 15(4), 508-524.
[25] Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., Shekelle, P., Stewart, L. A., & Group, P. (2015). Preferred reporting items for systematic review and meta-analysis protocols ( PRISMA-P ) 2015 statement. System Reviews, 4(1), 1-9.
[26] Oberlin, L. E., Waiwood, A. M., Cumming, T. B., Marsland, A. L., Bernhardt, J., & Erickson, K. I. (2017). Effects of Physical Activity on Poststroke Cognitive Function A Meta-Analysis of Randomized Controlled Trials. Stroke, 48(11), 3093-3100. https://doi.org/10.1161/STROKEAHA.117.017319
[27] Ozdemir, F., Birtane, M., Tabatabaei, R., Kokino, S., & Ekuklu, G. (2001). Comparing stroke rehabilitation outcomes between acute inpatient and nonintense home settings. Archives of Physical Medicine and Rehabilitation, 82(10), 1375-1379. https://doi.org/10.1053/apmr.2001.25973
[28] Pereira, A. C., Huddleston, D. E., Brickman, A. M., Sosunov, A. A., Hen, R., Mckhann, G. M., Sloan, R., Gage, F. H., Brown, T. R., & Small, S. A. (2007). An in vivo correlate of exercise-induced neurogenesis in the adult dentate gyrus. Proceedings of the National Academy of Sciences of the United States of America, 104, 5638-5643.
[29] Quaney, B. M., Boyd, L. A., McDowd, J. M., Zahner, L. H., Jianghua He, Mayo, M. S., & MacKo, R. F. (2009). Aerobic exercise improves cognition and motor function poststroke. Neurorehabilitation and Neural Repair, 23(9), 879-885. https://doi.org/10.1177/1545968309338193
[30] Rosenthal, R. (1979). The file drawer problem and tolerance for null results. Psychological Bulletin, 86(3), 638-641. https://doi.org/10.1037/0033-2909.86.3.638
[31] Solà-Serrabou, M., López, J. L., & Valero, O. (2019). Effectiveness of training in the elderly and its impact on health-related quality of life. Apunts Educacion Física y Deportes, 137, 30-42. https://doi.org/10.5672/APUNTS.2014-0983.CAT.(2019/3).137.03
[32] Studenski, S., Duncan, P. W., Perera, S., Reker, D., Lai, S. M., & Richards, L. (2005). Daily functioning and quality of life in a randomized controlled trial of therapeutic exercise for subacute stroke survivors. Stroke, 36(8), 1764-1770. https://doi.org/10.1161/01.STR.0000174192.87887.70
[33] Sun, J., Ke, Z., Yip, S. P., Hu, X., Zheng, X., & Tong, K. (2014). Rehabilitation Outcome after Stroke by BDNF Upregulation and Stress Suppression. BioMed Res, Article ID, 1-8.
[34] Tang, A., Eng, J. J., Krassioukov, A. V., Tsang, T. S. M., & Liu-Ambrose, T. (2016). High-and low-intensity exercise do not improve cognitive function after stroke: A randomized controlled trial. Journal of Rehabilitation Medicine, 48(10), 841-846. https://doi.org/10.2340/16501977-2163
[35] Tsai, C., Wang, C., Pan, C., & Chen, F. (2015). The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Frontiers in Behavioral Neuroscience, 9(23), 1-12. https://doi.org/10.3389/fnbeh.2015.00023
[36] Vanderbeken, I., & Kerckhofs, E. (2016). A systematic review of the effect of physical exercise on cognition in stroke and traumatic brain injury patients. NeuroRehabilitation, 40(1), 33-48. https://doi.org/10.3233/NRE-161388
[37] Wagle, J., Farner, L., Flekkøy, K., Bruun, W., Sandvik, L., Fure, B., Stensrod, B., & Engedel, K. (2011). Early Post-Stroke Cognition in Stroke Rehabilitation Patients Predicts Functional Outcome at 13 Months. Dement Geriatr Cogn Disord, 31, 379-387. https://doi.org/10.1159/000328970
[38] Winter, B., Breitenstein, C., Mooren, F. C., Voelker, K., Fobker, M., Lechtermann, A., Krueger, K., Fromme, A., Korsukewitz, C., Floel, A., & Knecht, S. (2007). High impact running improves learning. Neurobiology of Learning & Memory, 87, 597-609. https://doi.org/10.1016/j.nlm.2006.11.003
[39] Yeh, T.-T., Chang, K.-C., & Wu, C.-Y. (2019). The Active Ingredient of Cognitive Restoration: A Multicenter Randomized Controlled Trial of Sequential Combination of Aerobic Exercise and Computer-Based Cognitive Training in Stroke Survivors With Cognitive Decline. Archives of Physical Medicine and Rehabilitation, 100(5), 821-827. https://doi.org/10.1016/j.apmr.2018.12.020
ISSN: 2014-0983
Received: January 20, 2021
Accepted: April 12, 2021
Published: October 1, 2021
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


