Multisystem Aquatic Therapy and Emotional Regulation in Students with Autism Spectrum Disorder
Elena Conde-Pascual
Rafael Román-Noguerol
Fernanda Borges-Silva
*Corresponding author: Fernanda Borges-Silva bsfernanda@ucam.edu
Cite this article
Conde-Pascual, E., Román-Noguerol, R., & Borges-Silva, F. (2026). Multisystem aquatic therapy and emotional regulation in students with Autism Spectrum Disorder. Apunts. Educación Física y Deportes, 164, 47-60. https://doi.org/10.5672/apunts.2014-0983.es.2026.164.05
Abstract
It has been shown that aquatic interventions promote significant improvements in psychomotor skills in children with Autism Spectrum Disorder (ASD), although further research is required to confirm their effectiveness in different contexts. Therefore, the objective of this study was to examine the impact of Multisystem Aquatic Therapy (CI-MAT) on aquatic skills and emotional regulation in children diagnosed with ASD in the school context. A sample of 14 children (N = 14) was included, comprising 9 boys (64.3%) and 5 girls (35.7%), aged between 7 and 11 years (M = 8.93; SD = 1.439). With respect to severity levels, 8 children were diagnosed at level 1 (57.1%) and 6 at level 2 (42.8%). The intervention lasted 24 sessions of 40 minutes each, over a period of 12 weeks (two per week). In the experimental group (8 participants, 4 with ASD level 1 and 4 with ASD level 2), the CI-MAT program was implemented, whereas the control group (6 participants, 4 with ASD level 1 and 2 with ASD level 2) did not carry out any type of activity in the aquatic environment. To assess emotional regulation, the Spanish version of the Emotional-Regulation Skill Questionnaire (ERSQ) was used. The Aquatic Skills Checklist (ASC) was used to assess skill development. The principal researcher and an assistant recorded the data directly on the assessment instruments, given the need to ensure recording reliability and to overcome the self-assessment difficulties that children with ASD might present. The results showed that the CI-MAT program had significant effects on improving aquatic skills, as well as emotional regulation, and is therefore presented as a resource to be considered in the educational context for working with children diagnosed with ASD.
Introduction
According to the World Health Organization (WHO) (2022), Autism Spectrum Disorder (ASD) is understood as a persistent difficulty in the process of socialization, together with a restricted pattern of interests and sensory limitations. In turn, recent studies (Garrido-Torres et al., 2024; Cuellar-Salazar, 2024; Cano-Villagrasa & López-Zamora, 2024) define ASD as a neurodevelopmental disorder, with complex clinical manifestations that arise between 18 and 36 months of age. For these authors, and in line with what is established by the WHO, children with autism are characterized by deficits in social interaction, a restricted range of interests, and repetitive stereotyped behaviors.
This disorder presents complex dysfunctions in the development of the nervous system, manifesting in the early stages of life (González de Rivera Romero et al., 2022). With regard to the educational context, in 2018 it was estimated that the global incidence of ASD among the child population in Spain reached 15.5 per 1,000 preschool children and 10 per 1,000 school-aged children (Morales-Hidalgo et al., 2018).
For children with ASD, participation in physical activities plays a fundamental role in improving socialization (Ketcheson et al., 2017). More recent studies, such as that of López-Díaz et al. (2021), show how physical activity not only contributes to physical well-being, but also positively affects mental health, social interaction, and emotional adaptation. In addition, according to Gómez et al. (2018), physical activity is one of the key dimensions when it comes to achieving a good quality of life in people with ASD, as it allows for the development of motor skills and the generation of positive psychological contexts, as well as behavioral changes.
At present, the lack of physical activity in children with Autism Spectrum Disorder (ASD) is a global phenomenon with significant consequences for their development. In this context, it is essential to analyze the effects of physical activity in the motor, behavioral, and emotional domains of children with ASD, as well as to identify valid strategies to enhance these benefits. According to authors such as Fernández-Díaz et al. (2023), following a plan of 30 minutes of daily moderate physical activity and a healthy lifestyle entails notable benefits and improvements in the behavior and conduct of children with ASD.
At the behavioral level, it has been shown that physical activity reduces levels of aggressiveness, irritability, and depression, while at the same time an increase in self-esteem, social interaction, and communication skills is observed. Along the same lines, Fessia et al. (2018) observed that physical activity is a unique tool for achieving behavioral changes in children with ASD.
In this context, one of the main characteristics to be addressed in the educational setting with this type of student is impulsivity and the inability to control emotions (Márquez et al., 2023). Hassen et al. (2023) define emotional regulation as the ability of a person to understand, express, and manage their own emotions appropriately, as well as to interpret and respond to the emotions of others.
According to van’t Hooft et al. (2024), activities in the aquatic environment can promote aquatic competence, emotional regulation, and certain social behaviors in schoolchildren with ASD; however, larger and more controlled studies are required to confirm these effects. Pan (2010) argues that the implementation of an exercise program in the aquatic environment allows children with ASD to improve their sensory and motor function.
Caputo et al. (2018) applied the CI-MAT program (Comprehensive Multisystem Aquatic Therapy), which is structured in progressive phases in order to facilitate the adaptation of children with ASD to the aquatic environment. In a first stage, the program focuses on emotional bonding and affective safety, taking advantage of the characteristic attachment behavior of these children to establish physical contact with the therapist in the water. Once this relationship of trust has been consolidated, instruction in aquatic and swimming skills is introduced through exercises specifically adapted to their needs and motor limitations. Finally, the program incorporates a dimension of social integration, fostering interaction and cooperation with peers during activities in the aquatic environment. Overall, this multisystem methodology not only addresses the emotional and social needs of children but also shows promise in promoting improvements in their motor skills.
Among the aquatic intervention protocols considered to be of greatest relevance in the therapeutic field is the so-called Halliwick Therapy, which constitutes a structured, gradual, and objectively measurable program designed to promote the development of fundamental aquatic skills such as postural control, balance, breathing, and locomotion (Vodakova et al., 2022).It was created by McMillan (1977) to teach swimming to people with physical disabilities and, over time, evolved into a broader therapeutic intervention. According to various studies on the subject (Aleksandrovic et al., 2015; Naumann et al., 2021), most of the interventions proposed in the aquatic environment for children with ASD are aimed at improving their motor skills and aquatic skills, but there are few protocols that address aspects related to the regulation of their emotions.
Based on the above, there is a need to further develop an integral intervention approach, such as Multisystem Aquatic Therapy, which combines emotional, motor, social, and functional learning components organized in phases, in order to promote adaptation, skill development, and the inclusion of children with ASD. The present study aims to examine whether Multisystem Aquatic Therapy (CI-MAT) produces significant improvements in aquatic skills and emotional regulation in children with ASD in the school context.
Method
The present study adopted a quantitative approach, employing a quasi-experimental two-group design with pretest and posttest measures and a systematic observational record of participants’ behaviors, following the model of Alaniz et al. (2017). Changes were evaluated after the intervention applied to the experimental group and in comparison with the control group, while specific behaviors of interest were documented during the intervention. The study included one independent variable: an aquatic physical activity program (CI-MAT), and two dependent variables: emotional regulation and aquatic skills.
Participants
A total of 14 children (N = 14) participated in this study, of whom 9 were boys (64.3%) and 5 were girls (35.7%), aged between 7 and 11 years (M = 8.93; SD = 1.439). These students were enrolled in third grade (n = 5), fourth grade (n = 5), and sixth grade of primary education (n = 4). The inclusion criteria were: 1) having a diagnosis of ASD, level 1 (“requires support”) or 2 (“requires substantial support”), according to the DSM-5 diagnostic criteria guidelines (American Psychiatric Association, 2014); 2) not having any disabling condition that would prevent participation in physical activity; and 3) not having previously participated in the CI-MAT program. Prior to the intervention, comparisons were conducted between the experimental group and the control group on pre-intervention scores across all dimensions to verify baseline equivalence. No significant differences were found (p > .05), indicating that the groups were comparable at the beginning of the study.
Group assignment was carried out by convenience sampling, balancing severity levels. The experimental group, which worked through the CI-MAT program, consisted of 8 participants (6 boys and 2 girls, 4 with ASD level 1 and 4 with ASD level 2), whereas the control group, in which no intervention was carried out, was composed of 6 participants (3 boys and 3 girls, 4 with ASD level 1 and 2 with ASD level 2 (Table 1).
It is necessary to clarify that in the present study the term level is used to refer to ASD severity, in accordance with the DSM-5 classification, which distinguishes three levels of support. The use of the term grade is avoided, as it is less precise in the diagnostic field. Children with level 1 present good overall functioning with mild social difficulties and rigidity in their behaviors; at level 2, these difficulties are more marked and affect autonomy; and at level 3, limitations are very severe and require very substantial support. Only children with levels 1 and 2 participated in the study, as they presented sufficient functioning to take part in the proposed measurements and tasks (American Psychiatric Association, 2014; Lord et al., 2018).
The parents or legal guardians of the participants signed an informed consent form to participate and were informed of the objectives and characteristics of the study. All procedures were carried out with the approval of the ethics committee of the Catholic University of Murcia, reference code CE012417.
Instruments
To assess children’s emotional regulation, the Spanish version by Para conocer la regulación emocional de los niños, se utilizó la versión en español de Orozco-Vargas et al. (2021) of the original Emotional-Regulation Skill Questionnaire (ERSQ) by Berking and Znoj (2008) was used, which is characterized by evaluating a broad spectrum of adaptive skills for successful emotion regulation. The ERSQ is an instrument composed of 27 items that uses a 4-point Likert-type response format ranging from 0 (“not at all”) to 4 (“almost always”). It includes nine dimensions (Emotional awareness, Sensation, Clarity, Knowledge, Acceptance, Tolerance, Self-support, Willingness to confront, and Modification) through which cognitive and behavioral strategies are measured. The ERSQ has been used to investigate emotional regulation both in the general population and in clinical populations, specifically in different studies with autistic children (Hendrix et al., 2022; Butterworth et al., 2014). In the present study, the questionnaire was administered by the principal researcher, with the support of another trained researcher, to both the experimental group and the control group, before and after the aquatic intervention. The evaluators received prior training of 6 hours on the correct formulation of the items and the recording of responses. Inter-rater agreement was evaluated in a subsample (0.88 Kappa), indicating high reliability. To ensure comprehension of each item, the researchers asked the questions directly to the children and completed the questionnaire on their behalf, ensuring the reliability and validity of the responses (Table 2).
Table 2
Dimensions and skills assessed by the Emotional-Regulation Skill Questionnaire (ERSQ)
The Aquatic Skills Checklist (ASC) was used to assess skill development, a tool based on the American Red Cross Water Safety Instructor Manual (2009). This checklist assesses 13 swimming skills: movement in the water, breath control, propulsion, exiting the water, back floating, and turns, among others. Each skill was rated on a scale from zero to three (0: unable to complete the skill; 1: skill completed with physical assistance from the therapist; 2: skill completed with a flotation device; 3: skill completed independently). Participants could obtain a maximum score of 39 points for the total ASC score (Table 3). The ASC was used as a performance observation tool to record the presence/absence (or level) of the indicated aquatic skills. Although the ASC checklist is widely used in training programs, no published evidence of a complete psychometric validation was found. Therefore, in this study, the ASC was used as an operational working tool for skill assessment, and the results are interpreted within that context. The evaluators received prior training of 4 hours on scale administration and item coding. Inter-rater reliability, evaluated using Kappa, was 0.87, and assessments were conducted blind to participants’ group assignment.
Studies such as those by Alaniz et al. (2017) and Lawson et al. (2014) also used this tool to assess students’ swimming skills. Data collection was conducted before and after the intervention through direct observation of aquatic skills. The researchers used the checklist as a standardized record to document the level of development of these skills.
Procedure
The intervention carried out with the CI-MAT program is detailed below. Children who met the established participation criteria completed a total of 24 sessions of 40 minutes each over a period of 12 weeks (two per week). Students were divided into two groups: experimental and control. In the experimental group (8 participants), the CI-MAT program was implemented, whereas the control group (6 participants) did not perform any aquatic activity, following their normal school routine with physical education classes (Figure 1).
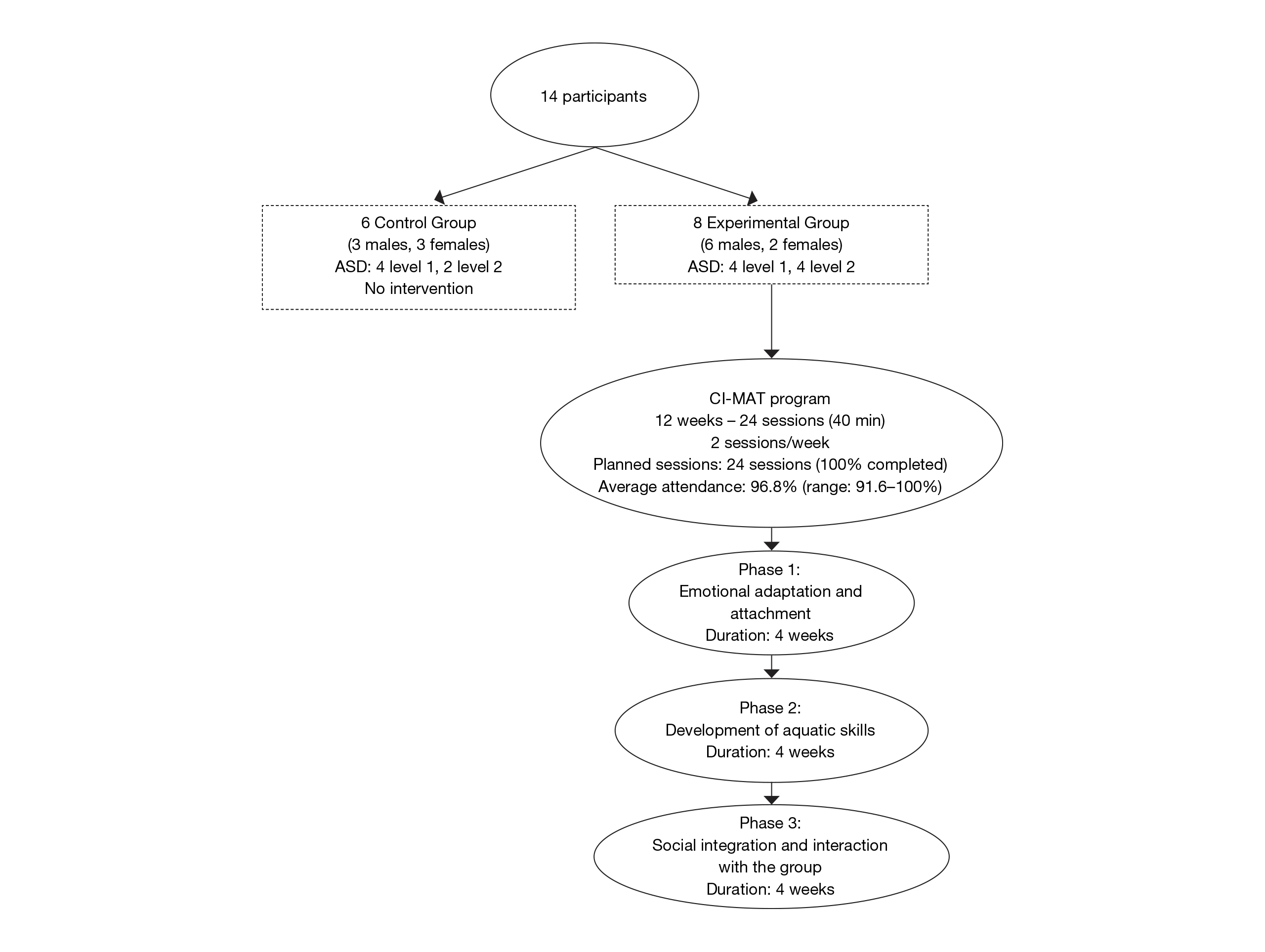
The three phases of this program (emotional adaptation and creation of attachment to the instructor; development of aquatic skills; and social integration phase) were divided equally, with 4 weeks allocated to each phase. Average attendance at the sessions was 96.8% (range 91.6–100%). All scheduled sessions were completed.
In the first phase (emotional adaptation and creation of attachment to the instructor), students with ASD worked apart from the rest of the class, interacting exclusively with the instructor, although they shared the aquatic space with the other classmates, who were led by another instructor. Some examples of the activities carried out are shown in Table 4.
Table 4
Examples of aquatic activities applied according to the CI-MAT model for children with ASD
In the second phase (development of aquatic skills), progressive work related to motor difficulty and autonomy in the aquatic environment was initiated. The first sessions were conducted with physical contact with the instructor, who assisted the student with ASD in performing activities such as floating, turning, moving in the water while floating in the prone position, and moving to retrieve non-submersible materials or to exit the pool. In the final sessions of this second phase, the aim was for participants to be able to move in the water without assistance or physical contact with the instructor, as well as to be able to submerge to retrieve submersible materials from the bottom of the pool and to be autonomous when exiting the water when instructed by the instructor (examples of activities carried out are shown in Table 4).
Third, the social integration phase was reached, in which students with ASD were included within the class group. Previously, the student with ASD and the instructor worked in the same space as the rest of the class but without direct interaction with the other classmates; from that moment on, the student with ASD began to share space and interactions with the rest of the class (students without ASD). Examples of the activities carried out are shown in Table 4.
To increase the reliability of measurement with the ASC, the tests were independently evaluated by two trained evaluators. Inter-rater agreement was calculated, and disagreements were resolved through joint review. Likewise, a pilot test was conducted to ensure the applicability of the items to the study population. The questionnaire was administered by the principal researcher and a trained research assistant to both the experimental group and the control group in a quiet, noise-free location. It was administered before the usual physical activity practice, prior to the start of the aquatic intervention, and again at the end of the intervention, after the 12-week period. The researchers completed the questionnaire after asking the children about each item, with the aim of helping them better understand its content. Emphasis was placed on response anonymity, voluntariness, and the need for participants to respond as honestly as possible. The time required to complete all scales was approximately 15 minutes; it varied slightly depending on the participant.
The Aquatic Skills Checklist (ASC) was also administered by the principal researcher and the research assistant. Data collection was conducted before and after the intervention through direct observation of aquatic skills. The researchers used the checklist as a standardized record to document the level of development of these skills.
The intervention was carried out in the school environment, which included children with and without ASD. Children without ASD were not included in the research data. Both the principal researcher and the research assistant held degrees in Physical Activity and Sport Sciences and had prior training in multisystem aquatic methodology. It is important to note that they had previous experience as swimming instructors for students with ASD.
Statistical Analysis
Statistical analysis was performed using the SPSS package for Windows (version 27.0; IBM). Before the intervention, equivalence between the experimental and control groups was examined using independent-samples t tests across all variables, in order to ensure baseline comparability. This verification made it possible to attribute subsequent changes more confidently to the intervention rather than to prior differences between groups.
With regard to emotional regulation, descriptive statistics of pretest and posttest scores for both groups were obtained to contextualize participants’ initial status. Subsequently, ERSQ questionnaire items were examined and grouped according to the theoretical dimensions of the instrument, calculating composite scores by dimension and a total score. In the experimental group, paired-samples t tests were applied to evaluate the effect of the CI-MAT program on emotional regulation, while equivalent tests were applied in the control group to analyze natural evolution without intervention. Next, intergroup comparisons were conducted using independent-samples t tests on posttest scores to determine whether the observed improvements could be attributed to the program. In all analyses, 95% confidence intervals, effect sizes (Cohen’s d and Hedges’ g), and bootstrap estimates were calculated.
With regard to aquatic skills, individual differences (pre–post) were calculated for each item of the ASC instrument, and total scores per participant were obtained. Subsequently, a mixed repeated-measures ANOVA was applied with one within-subject factor (Time: pre–post) and one between-subject factor (Group: experimental–control). The primary focus was on the Time × Group interaction as an indicator of the effectiveness of the CI-MAT program in the development of aquatic skills. Partial η² was reported as a measure of effect size.
Finally, a priori statistical power was calculated using the G*Power program (paired-samples t test, expected medium effect size d = 0.5, α = .05, power = .80), which indicated a minimum sample size of 34 participants. However, the available sample consisted of 14 students, which reduces statistical power and limits the generalizability of the results. Nevertheless, the findings provided preliminary evidence of the effectiveness of the CI-MAT program, which should be confirmed in studies with larger samples.
Results
CI-MAT and emotional regulation
Before the intervention, baseline equivalence between the experimental and control groups was assessed across all ERSQ dimensions using independent-samples t tests. The results indicated that no statistically significant differences were observed in any dimension (t(12) < 1.25, ps > .23; 95% CI via bootstrap [–3.34, 1.88]), suggesting that both groups were comparable at the beginning of the study. This initial equivalence made it possible to attribute subsequent changes more confidently to the intervention rather than to prior differences between groups (see Table 5).
Table 5
Comparison of means and standard deviations of ERSQ dimensions between groups before the intervention
Data normality was tested using the Shapiro–Wilk test in both the experimental group and the control group. Both in the pretest (experimental: p = .359; control: p = .748) and in the posttest (experimental: p = .869; control: p = .926), data followed a normal distribution, considering a significance level of α = .05. With regard to intragroup analysis, in the experimental group, the paired-samples t test showed a significant increase in scores after the intervention (Pre: M = 26.50, SD = 5.32; Post: M = 34.63, SD = 5.40), t(7) = −10.94, p < .001. The mean difference was 8.13 points (95% CI = 6.37, 9.88), with a very large effect size (Hedges’ g = 3.87), indicating a substantial improvement in emotional regulation. In the control group, the intragroup comparison showed no significant differences (Pre: M = 25.50, SD = 8.48; Post: M = 26.50, SD = 6.63), t(5) = −0.968, p = .377, with a mean difference of 1 point (95% CI = −3.65, 1.65), indicating that no relevant changes occurred without intervention.
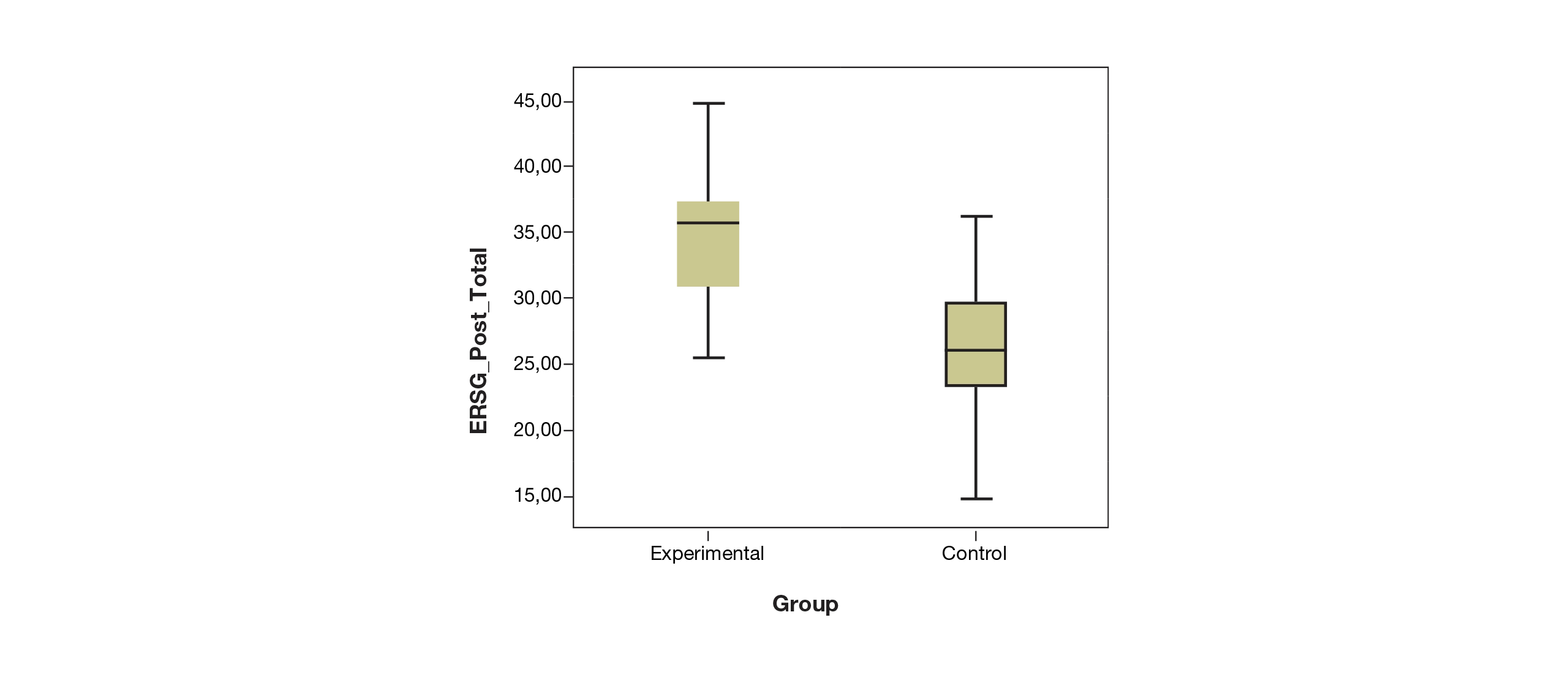
For the post-intervention intergroup comparison, an independent-samples t test was conducted to compare posttest data between the experimental group and the control group. Levene’s test indicated homogeneity of variances (F = 0.066, p = .802). The results showed that the experimental group obtained significantly higher posttest values (M = 34.63, SD = 5.40) than the control group (M = 26.50, SD = 6.63), t(12) = 2.533, p = .026, with a mean difference of 8.13 points (95% CI = 1.14, 15.11). The effect size was very large (Cohen’s d = 1.35), evidencing a substantial effect of the intervention on emotional regulation (Table 6).
Table 6
Descriptive statistics and comparison of total emotional regulation scores (Pre and Post) for the experimental and control groups
As shown in Table 6, the experimental group increased its scores from 26.50 (SD = 5.32) at the pre-intervention measurement to 34.63 (SD = 5.40) at the post-intervention measurement, with a mean difference of 8.13 points (95% CI [6.37, 9.88]) and a very large effect size according to Hedges’ g = 3.87. In contrast, the control group showed a non-significant change, increasing from 25.50 (SD = 8.48) to 26.50 (SD = 6.63), with a mean difference of 1.00 point (95% CI [–3.65, 1.65]). The post-intervention comparison between groups confirmed the effectiveness of the intervention, showing a mean difference of 8.13 points (95% CI [1.14, 15.11]) in favor of the experimental group, with a large effect size according to Cohen’s d = 1.35. These results indicate that the swimming program significantly improved emotional regulation in children in the experimental group, whereas no relevant changes were observed in the control group (Figure 2).
After the global analysis of emotional regulation, the nine dimensions into which the ERSQ is divided were examined in order to identify which specific aspects showed significant changes, thereby allowing a more detailed interpretation of the effects of the CI-MAT program. Pre–post comparisons in the experimental group showed improvements across all dimensions which are significant in Knowledge (Pre: M = 1.25, SD = 0.79; Post: M = 2.50, SD = 0.99; t(7) = -4.26, p = 0.004) and Acceptance (Pre: M = 1.79, SD = 0.85; Post: M = 2.79, SD = 0.71; t(7) = -4.58, p = 0.003), whereas other dimensions such as Emotional awareness, Sensation, Clarity, Tolerance, Self-support, Willingness to confront, and Modification showed moderate increases, although not statistically significant. In contrast, the control group did not present relevant changes in any dimension between pre-intervention and post-intervention, indicating that the improvements observed in the experimental group are attributable to the intervention. The post-intervention intergroup comparison showed significant differences in favor of the experimental group in Willingness to confront (Experimental: M = 3.46, SD = 0.89; Control: M = 2.17, SD = 0.46; t = 3.53, p = .005) and positive trends in Knowledge (p = .078) and Acceptance (p = .072), whereas the remaining dimensions presented higher scores in the experimental group without reaching statistical significance. These results show that the CI-MAT program primarily favored the ability to confront emotions, as well as emotional identification and acceptance, and generated moderate improvements in other emotional regulation skills.
Repeated-measures analyses (group × time ANOVA) showed differential effects in three ERSQ dimensions. In Knowledge (F(1.12) = 8.72, p = .012), the experimental group increased from M = 1.25 to 2.50, whereas the control group remained unchanged. In Acceptance (F(1.12) = 7.98, p = .015) and Confrontation (F(1.12) = 10.34, p = .007), significant improvements were also observed in the experimental group compared with the stability of the control group. The remaining dimensions did not reach statistical significance (p > .05), although some showed increasing trends in the experimental group.
Overall, these findings indicate that the CI-MAT program had a differential and significant effect on the Knowledge, Acceptance, and Willingness to confront dimensions, whereas the remaining dimensions remained relatively stable; this suggests that the intervention specifically impacted key areas of emotional regulation in the participants.
Table 7
Pre-intervention and post-intervention results by dimension in the experimental and control groups, intragroup differences, and post-intervention comparison
CI-MAT and aquatic skills
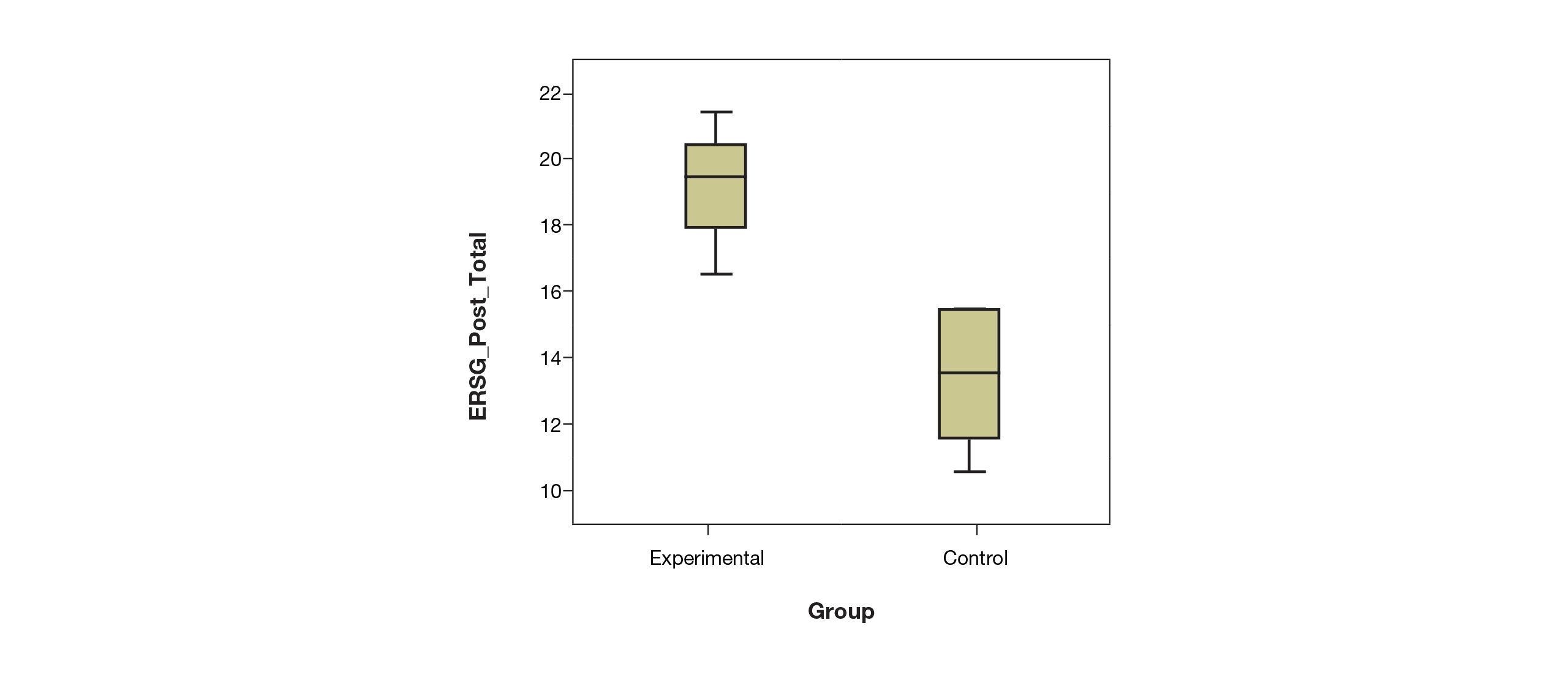
Total ASC scores were analyzed before and after the intervention with the CI-MAT program. The experimental group showed a significant increase in total ASC scores after the CI-MAT intervention, increasing from 13.88 ± 1.96 at pre-assessment to 19.75 ± 1.75 at post-assessment, with a mean change of 5.87 points, whereas the control group showed a much smaller increase, from 13.00 ± 2.37 to 13.83 ± 2.14, with a mean change of 0.83 points. The Time × Group interaction of the mixed repeated-measures ANOVA was significant (F = 25.47, df = 1.12, p < .05, partial η² = 0.70), indicating that improvement in the experimental group was significantly greater than in the control group. Pre- and post-scores showed an approximately normal distribution (Shapiro–Wilk, p > .05), which supports the use of parametric analysis to evaluate the effectiveness of the program (Table 8).
Therefore, the implementation of the CI-MAT program was associated with significant increases in emotional regulation and aquatic skills in the experimental group, in contrast to the stability observed in the control group.
Discussion
In this study, the effects of a Multisystem Aquatic Therapy (CI-MAT) program on emotional regulation and aquatic skills in children with ASD aged between 7 and 11 years were investigated. The results obtained show clear agreement with the existing scientific literature, reinforcing the idea that Multisystem Aquatic Therapy can be a useful tool for improving emotional regulation and motor skills in children with autism.
The results of the present study, which show a significant improvement in emotional regulation in the experimental group, are consistent with studies such as those by Battaglia et al. (2019), Lourenço et al. (2016) and Bernate et al. (2024), who state that physical exercise promotes emotional regulation in people with autism. Likewise, according to Battaglia et al. (2019), the aquatic environment helps people with autism improve their emotional regulation. These authors agree that the aquatic environment is particularly beneficial for people with autism. Water, by offering a unique sensory environment, can help calm and modulate emotional responses. Buoyancy reduces the force of gravity and provides constant proprioceptive feedback, which can have a calming and organizing effect on the nervous system.
In particular, the CI-MAT program produced significant improvements in the dimensions of Knowledge, Acceptance, and Willingness to confront (Berking & Znoj, 2008; Orozco-Vargas et al., 2021), evidencing a positive impact on the identification, understanding, and coping with emotions. The increase in Knowledge is consistent with what was proposed by Lourenço et al. (2016), who highlight that structured physical activity promotes self-perception and emotional recognition in people with ASD. With regard to Acceptance, the results are consistent with the findings of Caputo et al. (2018) and Naumann et al. (2021), who demonstrated that aquatic programs facilitate emotional regulation by promoting a safe and predictable environment that reduces avoidance and fosters acceptance of affective states. Finally, the improvement observed in the Willingness to confront dimension is related to the results of Battaglia et al. (2019) and Bernate et al. (2024), in which participation in aquatic and physical exercise programs increased the ability to cope with challenging emotional situations, strengthening self-efficacy and goal-directed behavior.
Overall, these findings are consistent with those reported by Zanobini and Solari (2019) and van’t Hooft et al. (2024), who emphasize that aquatic interventions contribute to emotional development in people with ASD, reinforcing the usefulness of CI-MAT in improving emotional skills. According to the systematic review by Ferreira et al. (2021), it is shown that there are various protocols and activities that help improve emotional regulation in children with autism; however, among them, the aquatic environment stands out as a fundamental element, as in addition to behavioral benefits it also provides physical and motor benefits (Lourenço et al., 2016; Yilmaz et al., 2010).
When analyzing aquatic skills after the application of the CI-MAT program, a substantial improvement in the aquatic competencies of participants with ASD was evidenced. This finding is in line with that described by Pan (2010), who reported that structured swimming programs significantly improve aquatic skills and autonomy in children with ASD.
Similarly, Alaniz et al. (2017) demonstrated that group aquatic therapy increases water safety and motor competence, which has a positive impact on self-confidence and active participation. In addition, the improvement observed in the present research is consistent with the systematic review by Aleksandrovic et al. (2016), which confirms the positive effects of aquatic activities on physical condition and the acquisition of skills in the aquatic environment in this population.
The methodological approach of the CI-MAT program shares foundations with the Halliwick method, described by McMillan (1977) and standardized by the American Red Cross (2009), which promotes aquatic independence through balance control, rotation, and flotation in a safe and playful environment. In this regard, the improvements obtained reflect the effectiveness of progressive and individualized teaching strategies, principles consistent with those highlighted by Baena Beato et al. (2010), who emphasize the importance of structured guidance to promote motor learning in aquatic contexts.
Likewise, the findings are consistent with those of Battaglia et al. (2019) and Faraji et al. (2023), who observed significant improvements in gross motor skills and aquatic-specific skills following similar systematic interventions. Finally, these results support the conclusions of van’t Hooft et al. (2024) and Naumann et al. (2021), who highlight that adapted aquatic programs represent an effective means to improve motor competence, safety, and participation in people with ASD. Overall, the results of the present study confirm that the CI-MAT program, as a comprehensive aquatic intervention, promotes the development of functional skills and safe adaptation to the aquatic environment, providing children with greater control and autonomy (Yilmaz et al., 2010; Lara & Giménez, 2019)
In line with the results of this research, Caputo et al (2018) demonstrated how Multisystem Aquatic Therapy can be useful in improving motor deficits in people with autism, as well as in enhancing emotional regulation and aquatic skills. Multisystem Aquatic Therapy is not a one-dimensional intervention, but rather a holistic approach that can simultaneously benefit motor skills and emotional regulation, with a direct and measurable impact on the emotional well-being of participants.
Conclusions
The results of this study indicate that Multisystem Aquatic Therapy (CI-MAT) can contribute to improving emotional regulation and aquatic skills in children with ASD levels 1 and 2, aged between 7 and 11 years. Significant improvements were observed in Knowledge, Acceptance, and Willingness to confront, as well as in motor competence in the aquatic environment. These findings support the value of the aquatic environment as a setting that promotes both emotional and motor development.
However, given the limitation of the sample size, the results should be interpreted with caution, and future research with larger samples and longitudinal designs is recommended to confirm the effectiveness and stability of the observed effects. It would be interesting for future research to implement an active control and a follow-up period of 1 to 3 months post-intervention.
The ASC used does not have a published psychometric validation and was therefore treated as a performance observation tool. This limits the generalizability of the findings and their interpretation in terms of construct validity. Future studies are recommended to conduct formal validations (internal consistency, inter-rater reliability, construct validity, and test–retest reliability) of the ASC or to use validated instruments such as the SCAS or other validated analogues.
As a practical application, it is recommended that professionals adopt an integrated, progressive, and personalized intervention approach, in which the aquatic environment acts as a setting that enables the global development of children with ASD. To this end, it would be advisable to combine motor and emotional, cognitive, and social work, including moments of adaptation, exploration, and motor learning, while always maintaining a predictable and safe sequence that reduces anxiety and promotes confidence. It would be important to personalize objectives and strategies, taking into account the sensory profile, functional level, and learning style of each child, with adaptations that respect their communicative and motor needs. It is also suggested to promote the child’s participation in decision-making, positively reinforcing each achievement. Finally, it would be advisable to systematically record progress in both the motor and emotional domains in order to adjust interventions and evaluate effects in the short- and medium-term.
References
[1] Alaniz, M. L., Rosenberg, S. S., Beard, N. R., & Rosario, E. R. (2017). The effectiveness of aquatic group therapy for improving water safety and social interactions in children with autism spectrum disorder: A pilot program. Journal of Autism and Developmental Disorders, 47, 4006–4017. doi.org/10.1007/s10803-017-3264-4
[2] Aleksandrovic, M., Jorgic, B., Block, M., & Jovanovic, L. (2015). The effects of aquatic activities on physical fitness and aquatic skills in children with autism spectrum disorders: A systematic review. Facta Universitatis, Series: Physical Education and Sport, 13(3), 351–362.
[3] American Psychiatric Association (2014). Manual diagnóstico y estadístico de los trastornos mentales: DSM-5 (5.ª ed., versión en español). Editorial Médica Panamericana.
[4] American Red Cross (2009). American Red Cross Water Safety Instructor’s Manual. Mosby Lifeline.
[5] Baena Beato, P. A., Castilla Gutiérrez, N., & López Contreras, G. (2010). The Teaching Process of Autistic Children in a Water Environment. Apunts. Educación Física y Deportes, 101, 25–31. www.redalyc.org/articulo.oa?id=551656925004
[6] Battaglia, G., Agrò, G., Cataldo, P., Palma, A., & Alesi, M. (2019). Influence of a Specific Aquatic Program on Social and Gross Motor Skills in Adolescents with Autism Spectrum Disorders: Three Case Reports. Journal of Functional Morphology and Kinesiology, 4(2), 27. doi.org/10.3390/jfmk4020027
[7] Bernate, J. A., Salamanca, H. A. B., Roa, P. N. U., Rendon, R. D. D., Franco, I. P. F., & Fuentes, G. de J. A. (2024). Contribution of physical exercise on the emotional regulation of adults with autism spectrum disorder. Revista de Gestão Social e Ambiental, 18(2), e06910. doi.org/10.24857/rgsa.v18n2-145
[8] Berking, M., & Znoj, H. (2008). Entwicklung und Validierung eines Fragebogens zur standardisierten Selbsteinschätzung emotionaler Kompetenzen (SEK-27) [Development and validation of the Emotion Regulation Skills Questionnaire (ERSQ-27)]. Zeitschrift für Psychiatrie, Psychologie und Psychotherapie, 56(2). doi.org/10.1024/1661-4747.56.2.141
[9] Butterworth, T. W., Hodge, M. A., & Sofronoff, K. (2014). Validation of the emotion regulation and social skills questionnaire for young people with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44, 1535–1545. doi.org/10.1007/s10803-013-2014-5
[10] Cano-Villagrasa, A. & López-Zamora, M. (2024). Abordaje logopédico en los trastornos del neurodesarrollo. Editorial Tirant Lo Blanch. editorial.tirant.com/mex/libro/9788411836975
[11] Caputo, G., Ippolito, G., Mazzotta, M., Sentenza, L., Muzio, M. R., Salzano, S., & Conson, M. (2018). Effectiveness of a Multisystem Aquatic Therapy for Children with Autism Spectrum Disorders. Journal of autism and developmental disorders, 48, 1945–1956.
[12] Faraji, S., Najafabadi, M. G., Zandi, H. G., & Shaw, I. (2023). Effect of aquatic therapy on motor skill and executive function in children with autism spectrum disorder. South African Journal for Research in Sport, Physical Education and Recreation, 45(2), 17–27. doi.org/10.36386/sajrsper.v45i2.101
[13] Fernández-Díaz, M., Rodríguez-Fernández, J. E., López-García, S., & Rico-Díaz, J. (2023). Influence of physical activity on behavior and conduct in students with autism spectrum disorder in primary education: a systematic review. Revista Portuguesa de Educação, 36(1), e23011. doi.org/10.21814/rpe.26794
[14] Ferreira, B. P. G., Paz, C. L. da S. L., & Tenório, M. C. C. (2021). Water activities and social interaction of autistic children. RBPFEX - Revista Brasileira De Prescrição E Fisiologia Do Exercício, 14(90), 365–371. www.rbpfex.com.br/index.php/rbpfex/article/view/2032
[15] Fessia, G., Contini, L., Astorino, F. & Manni, D. (2018). Estrategias de actividad física planificada en autismo: revisión sistemática. Revista de salud pública (Bogotá, Colombia), 20(3), 390–395. doi.org/10.15446/rsap.v20n3.63040
[16] Garrido-Torres, N., Guzmán-Torres, K., García-Cerro, S., Pinilla Bermúdez, G., Cruz-Baquero, C., Ochoa, H., García-González, D., Canal-Rivero, M., Crespo-Facorro, B., & Ruiz-Veguilla, M. (2024). miRNAs as biomarkers of autism spectrum disorder: a systematic review and meta-analysis. European child & adolescent psychiatry, 33, 2957–2990. doi.org/10.1007/s00787-023-02138-3
[17] Gómez, L. E., Morán, L., Alcedo, M. A., Verdugo, M. Á., Arias, V. B., Fontanil, Y., & Monsalve, A. (2018). Escala KidsLife-TEA: evaluación de la calidad de vida de niños y adolescentes con trastorno del espectro del autismo y discapacidad intelectual. Salamanca, España: Instituto Universitario de Integración en la Comunidad. sid.usal.es/idocs/F8/FDO27385/Herramientas_15_2018.pdf
[18] González de Rivera Romero, T., Fernández-Blázquez, M. L., Simón Rueda, C., & Echeita Sarrionandia, G. (2022). Educación inclusiva en el alumno con TEA: una revisión sistemática de la investigación. Siglo Cero. Revista Española Sobre Discapacidad Intelectual, 53(1), 115–135. doi.org/10.14201/scero2022531115135
[19] Hassen, N. B., Molins, F., Garrote-Petisco, D., & Serrano, M. A. (2023). Emotional regulation deficits in autism spectrum disorder: The role of alexithymia and interoception. Research in developmental disabilities, 132, 104378. doi.org/10.1016/j.ridd.2022.104378
[20] Hendrix, N. M., Pickard, K. E., Binion, G. E., & Kushner, E. (2022). A systematic review of emotion regulation in parent-mediated interventions for autism spectrum disorder. Frontiers in psychiatry, 13. doi.org/10.3389/fpsyt.2022.846286
[21] Ketcheson, L., Hauck, J., & Ulrich, D. (2017). The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: A pilot study. Autism, 21(4), 481– 492. doi.org/10.1177/1362361316650611
[22] Lara, L. & Giménez, M. (2019). Aportes de intervención psicomotriz en multi-espacio (combinando medio acuático y sala), en abordaje de niños con autismo; estudio de casos. Revista iberoamericana de psicomotricidad y técnicas corporales, 44, 168–182. dialnet.unirioja.es/servlet/articulo?codigo=7274328
[23] Lawson, L. M., Foster, L., Harrington, M. C., & Oxley, C.A. (2014). Effects of a swim program for children with autism spectrum disorder on skills, interest, and participation in swimming. American Journal of Recreation Therapy,13(2), 17–27. doi.org/10.5055/ajrt.2014.0069
[24] López-Díaz, J. M., Moreno-Rodríguez, R. & López-Bastias, J. L. (2021). Análisis del impacto de un programa deportivo en niños con Trastorno del Espectro del Autismo. Retos digitales, 39, 98–105. dialnet.unirioja.es/servlet/articulo?codigo=7587475
[25] Lourenço, C., Esteves, D., & Corredeira, R. (2016). Potential Physical Activity in Individuals with Autism Spectrum Disorder. DESPORTO e Actividade Física para Todos, FPDD, 2(2), 31- 38 desportoeatividadefisicaparatodos-fpdd.org/potencialidades-da-atividade-fisica-em-individuos-com-perturbacao-do-espectro-do-autismo/
[26] Lord, C., Elsabbagh, M., Baird, G., & Veenstra-Vanderweele, J. (2018). Autism spectrum disorder. The Lancet, 392(10146), 508–520. doi.org/10.1016/S0140-6736(18)31129-2
[27] Márquez, E. P., Olivencia, J. J. L., & Mena, M. S. (2023). Support for the educational inclusion of students with Autism Spectrum Disorders (ASD) from the perspective of shadow teachers. Revista electrónica interuniversitaria de formación del profesorado, 26(1), 179–197. doi.org/10.6018/reifop.553511
[28] McMillan, J. (1977). The Halliwick method. Physiotherapy Journal, 63(11), 348–351.
[29] Morales-Hidalgo, P., Roigé-Castellví, J., Hernández-Martínez, C., Voltas, N., & Canals, J. (2018). Prevalence and Characteristics of Autism Spectrum Disorder Among Spanish School-Age Children. Journal of autism and developmental disorders, 48, 3176–3190. doi.org/10.1007/s10803-018-3581-2
[30] Naumann, K., Kernot, J., Parfitt, G., Gower, B. & Davison, K. (2021). Water-Based Interventions for People With Neurological Disability, Autism, and Intellectual Disability: A Scoping Review. Adapted Physical Activity Quarterly: APAQ , 38(3), 474–493. doi.org/10.1123/apaq.2020-0036
[31] Organización Mundial de la Salud (2022). Clasificación Internacional de Enfermedades, Undécima Revisión (CIE-11). icd.who.int/browse11
[32] Orozco-Vargas, A. E., García-López, G. I., Aguilera-Reyes, U., Venebra-Muñoz, A. (2021). Versión en Español del Emotion Regulation Skills Questionnaire: Análisis de su Fiabilidad y Validez. Revista Iberoamericana de Diagnóstico y Evaluación Psicológica. RIDEP, 4(61) 189-203.
[33] Ovsiannikov, E. Y., Koviazina, G. V., Poperekov, V. S., & Buldakova, N. V. (2019). Experimental Application of Hippotherapy Against Problems of Sensor Integration in Preschool Children with Autism Spectrum Disorders. Human. Sport. Medicine, 19(S2), 110–118. doi.org/10.14529/hsm19s215
[34] Pan C. Y. (2010). Effects of water exercise swimming program on aquatic skills and social behaviors in children with autism spectrum disorders. Autism : the international journal of research and practice, 14(1), 9–28. doi.org/10.1177/1362361309339496
[35] van ‘t Hooft, P., Moeijes, J., Hartman, C, van Busschbach, J. & Hartman, E. (2024). Aquatic Interventions to Improve Motor and Social Functioning in Children with ASD: A Systematic Review. Review Journal of Autism and Developmental Disorders. 1-21. doi.org/10.1007/s40489-024-00464-z
[36] Vodakova, E., Chatziioannou, D., Jesina, O. & Kudlacek, M. (2022). The Effect of Halliwick Method on Aquatic Skills of Children with Autism Spectrum Disorder. International journal of environmental research and public health,19(23), 16250. doi.org/10.3390/ijerph192316250
[37] Yilmaz, İ., Konukman, F., Birkan, B., & Yanardağ, M. (2010). Effects of Most to Least Prompting on Teaching Simple Progression Swimming Skill for Children with Autism. Education and Training in Autism and Developmental Disabilities, 45(3), 440–448. www.jstor.org/stable/23880116
[38] Zanobini, M., & Solari, S. (2019). Effectiveness of the Program “Acqua Mediatrice di Comunicazione” (Water as a Mediator of Communication) on Social Skills, Autistic Behaviors and Aquatic Skills in ASD Children. Journal of Autism and Developmental Disorders, 49, 4134–4146. doi.org/10.1007/s10803-019-04128-4
ISSN: 2014-0983
Received: June 16, 2025
Accepted: November 20, 2025
Published: April 1, 2026
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


