Effects of Light-Emitting Diode Therapy on Recovery of Adult Male Futsal Players
Victor Hugo de Freitas
Flavia Alessandra Guarnier
Thâmara Alves
Lúcio Flávio Soares-Caldeira
Alessandro Moura Zagatto
Solange de Paula Ramos
*Corresponding author: Solange de Paula Ramos solangedepaularamos@gmail.com
Cite this article
De Freitas, V.H., Guarnier, F.A., Alves, T., Soares-Caldeira, L.F., Moura Zagatto, A. & De Paula Ramos, S. (2021). Effects of Light-Emitting Diode Therapy on Recovery of Adult Male Futsal Players. Apunts Educación Física y Deportes, 146, 52-60.
https://doi.org/10.5672/apunts.2014-0983.es.(2021/4).146.06
Abstract
The aim of this study was to investigate the effects of light-emitting diode (LED) therapy on markers of physical performance, muscle damage, inflammation, and oxidative stress up to 24h post the Futsal-Specific Intermittent Shuttle Protocol (FISP). Ten adult futsal players performed the FISP seven days apart. Participants were randomized into two groups that received LED (630 nm; 300 mW; 4.6 J/cm2, 6 J per point, 120 J on each thigh) or Placebo. Heart rate (HR) and blood lactate concentration [Lac] were collected during the FISPs. Blood samples were collected for analysis of creatine kinase (CK), interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and advanced oxidation protein products (AOPP), and countermovement jump (CMJ) and perceived muscle soreness were assessed pre, post, and 24h post FISP. LED and Placebo groups presented similar mean HR (p = .58) and [Lac] (p = .86) during the FISPs. Interaction (p < .01) and time effects (p < .01) were observed for CK, with both Placebo (p < .01) and LED (p < .01) increasing CK at the post moment compared to pre. A time effect was found for CMJ (p < .01) and IL-6 (p < .01), showing that CMJ presented lower values at post (p < .01) and 24h post (p = .01) compared to the pre moment, and IL-6 increased at post compared to pre (p < .01) and returned to pre values 24h post FISP. Interaction, time, and group effects were not reported for muscle soreness, TNF-α, or AOPP (p > .05). In conclusion, LED therapy altered CK behavior post FISP, but did not change markers of physical performance, muscle soreness, inflammation, or oxidative stress of futsal players up to 24h post FISP.
Introduction
Futsal is a team sport, in which players cover 15% of total distance (~3000-4000 m) at high-intensity velocities (i.e. > 18.3 km h−1) (De Oliveira Bueno et al., 2014) and present heart rate (HR) values close to 86-90% of maximal HR (HRmax) during a match (Barbero-Alvarez et al., 2008; Castagna et al., 2009). Furthermore, constant sprints, abrupt stops, accelerations, changes of direction, and finalizations occur during matches (Naser et al., 2017). As a consequence of high-intensity physical and physiological demands, previous studies have reported decrements in physical performance during matches, as demonstrated by a lower distance covered at high intensity in the second half compared to the first (Barbero-Alvarez et al., 2008; De Oliveira Bueno et al., 2014; Milioni et al., 2016) and impaired knee flexor and extensor torque and lower-limb muscle power (inferred by countermovement jump test – CMJ) immediately (Dal Pupo et al., 2014) and up to 24h post-match (De Freitas et al., 2017). When consecutive matches are played, the same phenomenon is also observed on the following days (Freitas et al., 2014).
Exercise-induced muscle damage (EIMD) is frequently related to impaired performance immediately post and for some days after a futsal match (De Marchi et al., 2019; De Moura et al., 2012; Freitas et al., 2014). Previous studies have reported an increase in muscle damage, inflammation, and oxidative stress, indicated by increases in serum creatine kinase (CK) and lactate dehydrogenase (LDH) activities (De Marchi et al., 2019; De Moura et al., 2012), in interleukin 6 (IL-6) and C-reactive protein (CRP) (De Moura et al., 2012), and in carbonylated protein (CP) (De Marchi et al., 2019) levels immediately post and 48h post a futsal match. In this sense, strategies that accelerate the recovery of EIMD and physical performance are useful in assisting futsal players to reduce fatigue symptoms, leading to prompt availability of athletes for training sessions or competitions on days following matches.
Recently, the use of phototherapy has been suggested in sport with the main objective of promoting ergogenic effects, increasing physical performance during exercise, and as a recovery method after high intensity exercises, reducing EIMD in athletes of team and individual sports (Leal-Junior et al., 2015; Leal-Junior et al., 2019; Vanin et al., 2018). Phototherapy consists of applying light from red to near-infrared wavelengths emitted by low-density laser (Laser) or light-emitting diodes (LED) (Leal-Junior et al., 2019). Phototherapy stimulates cell photoreceptors in the mitochondrial respiratory chain of skeletal muscle, especially the enzyme cytochrome c oxidase (Hayworth et al., 2010). As a consequence, improvement in electron transference at the internal inner mitochondrial membrane can be seen, reducing the increased formation of reactive oxygen species (ROS), and enlarging the resultant intracellular adenosine triphosphate (ATP) pool (Hayworth et al., 2010). Improvement in the yield of total ATP production in skeletal muscle provides more available energy for muscle function, attenuating EIMD. A previous study suggested that phototherapy performed before futsal matches promoted a muscle protective effect, reducing muscle damage (i.e., CK and LDH) and oxidative stress (thiobarbituric acid reactive substances – TBARS and CP) markers of futsal players post and 48h post matches (De Marchi et al., 2019). However, it has not yet been reported whether phototherapy applied post-matches could be effective for accelerating recovery of futsal players. Furthermore, up to now, the effects of phototherapy on recovery markers of futsal players, including physical performance, up to 24h-post matches are still unknown. This information could assist coaches mainly in short tournaments, where the interval between matches is approximately 24h (Freitas et al., 2014).
The aim of this study was to investigate the effects of LED therapy on markers of physical performance, muscle damage, inflammation, and oxidative stress up to 24h post an exercise protocol that simulates the physical demands of futsal match-play. To justify the aim, we hypothesized that the exercise protocol performed could negatively affect EIMD associated markers of futsal players, similar to those reported post futsal (De Marchi et al., 2019; et al., 2012), and that LED may attenuate these negative effects.
Methods
Participants
Ten outfield players (age 23.5 ± 7.8 years, height 174.3 ± 6.1 cm, and weight 69.1 ± 3.8 kg), from an adult futsal team participated in the present study. This team was ranked in the second position from the access division (to the first division) of a State Futsal Championship. The sample was selected by convenience due to the limited number of players in a futsal team and the difficulty in finding different teams with the same training routine and schedule, with availability. The inclusion criteria were: playing for the team included in the present study; having trained in futsal for at least four years. All players were healthy, free of injury, and reported not having consumed ergogenic substances or anti-inflammatory drugs at the time of the experiment. In addition, all volunteer players were instructed not to consume alcohol or foods containing caffeine for at least 24h before performing the experimental procedures. The dietary intake was not guided by a nutritionist and no dietary recall was performed, however, players were instructed to eat regularly and hydrate frequently, voluntarily, and freely. Experimental procedures were conducted in the middle of the competitive season, in a moment of pause in the competitive calendar. The Ethics Committee on Research involving humans of the State University of Londrina (CAAE: 39519414.4.0000.5231; code granted: 930.218) approved the study, respecting the regulatory standards established by the National Health Council and according to the Declaration of Helsinki.
Procedures
To simulate the physical demands of futsal match-play, players performed the Futsal-Specific Intermittent Shuttle Protocol (FISP) (De Freitas et al., 2017). The FISP is a valid exercise protocol, allowing players to be homogeneously submitted to the physical demands of futsal matches. On the first experimental day, players arrived at the club at 9:00 a.m., without exercising for approximately 48h, for sample characterization (anthropometric measures: weight and height). Futsal players performed the FISP (De Freitas et al., 2017) seven days apart, at 2:00 p.m., on an official futsal court. Participants were randomized by a simple draw into two groups that performed LED or Placebo in a cross-over design (5 players underwent LED and 5 Placebo on the first day, being inverted on the second day). Although similar recovery effects are reported when using both LED and laser (Vanin et al., 2018), in the present study LED (non-coherent light source) was preferred due to the larger spot area, covering large skin areas at each point of light application. LED or Placebo conditions were applied approximately ~1-35 minutes after players completed the FISP and data collection. HR was monitored continuously and blood samples were collected from the earlobe after each block of FISP to analyze blood lactate concentration [Lac]. In addition, blood samples were collected before (pre), immediately post (post), and 24h post (24h) FISP to analyze the plasma concentration of CK, IL-6, tumor necrosis factor-alpha (TNF-α), and advanced oxidation protein products (AOPP). Pre and 24h post FISP, blood was collected before the warm-up. Pre and 24h post FISP, after the warm-up, and immediately post, the countermovement jump test (CMJ) was applied and perceived muscle soreness was monitored. The warm-up consisted of performing the FISP for 5 min with sprints at ~90% of maximal speed. This warm-up was also used to familiarize players with the FISP. To verify the maximal heart rate (HR), players performed the YO-YO intermittent recovery test level 1 (YO-YOIR1) (Bangsbo et al., 2008) one week prior to the first FISP, under exercise deprivation for approximately 48h. Experimental procedures were conducted in the middle of the competitive season, in a moment of pause in the competitive calendar.
Light-emitting diode therapy (LED) or Placebo
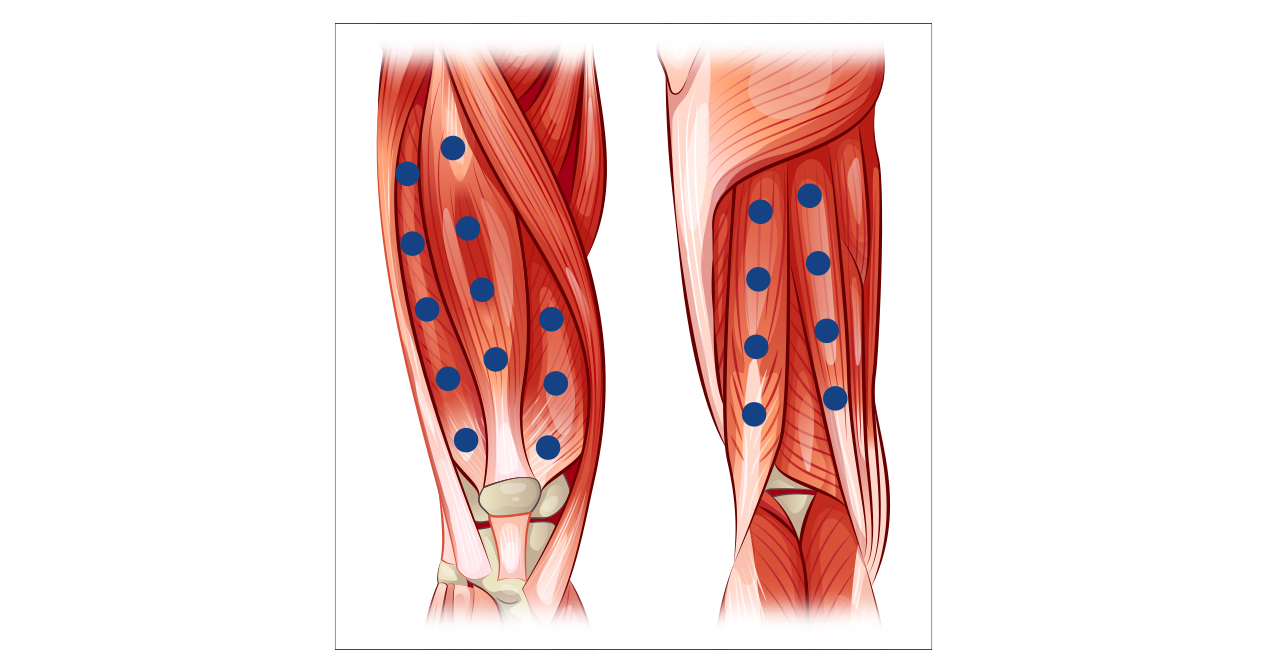
Light-emitting diode therapy (LED) or Placebo, were performed using commercial equipment (Table 1). The equipment was positioned on the quadriceps and hamstring muscles in contact with the skin, in accordance with Figure 1. At each point, 6 J of energy (20 s of application) were irradiated, totaling 120 J of energy applied on each thigh. The Placebo procedure was performed with the device switched off, without the players’ knowledge, as both groups (LED and Placebo) wore a blindfold when submitted to the protocol application. LED and Placebo were performed at the same anatomical sites and for a similar duration. LED wavelength and irradiated energy were performed in accordance with previous systematic reviews (Leal-Junior et al., 2015; Vanin et al., 2018). Before the experimental procedures, players of both groups (LED and Placebo) received an explanation about the effect of LED application, aiming to convince them that LED is effective to accelerate recovery.
Futsal-specific intermittent shuttle protocol (FISP)
The FISP consists of four blocks with a duration of 6 minutes per block, and five-minute intervals between blocks (totaling 39 min). The total distance covered during the FISP is 3600 meters and each exercise block is structured with 6 sequences of 10 displacements of 15 meters, in which players run at different intensities dictated by a beep and voice command. The sequence of displacements is: walking – 5.4 km/h; 2 x low-intensity running – 9 km/h; sprinting – maximal velocity; 2 x low-intensity running – 9 km/h; 2 x medium-intensity running – 13.5 km/h; high-intensity running – 18 km/h; walking – 5.4 km/h. The values of HR, changes in CMJ, perceived muscle soreness, and recovery markers of inflammation and oxidative stress in the FISP have been demonstrated to be similar to a simulated match (De Freitas et al., 2017).
Heart rate (HR)
HR was monitored at 1-s intervals using telemetric monitors (Polar®, RS800, Polar Electro, Finland). Mean HR was computed for the entire 4 blocks of the FISP (24 min = 4 x 6 min blocks). Furthermore, HR was measured in the YO-YOIR1, with the HR at the end of the test considered as maximal HR (HRmax). The percentage of HR monitored in the FISP, corresponding to HRmax (%HRmax), was also calculated.
Countermovement jump test (CMJ)
CMJ was performed using a contact mat (Smart Jump®, Fusion Sport, Australia). Players started the test in a standing position and performed a squat (~90º knee flexion) followed by a jump with hands placed on the hips. Players performed 3 maximal CMJ attempts with a 60s rest interval between attempts and the highest jump height was considered for analyses. The CMJ test presented an intra-class correlation coefficient (ICC) of 0.97 (Sattler et al., 2012).
Perceived muscle soreness
Muscle soreness was evaluated using a categorical scale (0-10) of pain (Cook et al., 1998). Players performed a ~90° knee flexion squat before reporting perceived muscle soreness on a scale, with 0 representing “no pain at all” and 10 “extremely intense pain, almost unbearable”. It is important to note that this variable was recorded by the same evaluator, one player at a time, in an isolated place without influence of other players.
Blood markers
5 ml blood samples were collected from an antecubital vein into heparinized tubes (Becton Dickinson, Franklin Lakes, USA). Samples were centrifuged (1370 g for 10 min at 4 °C) and the plasma collected was aliquoted and stored at −20 °C. Levels of IL-6 and TNF-α were determined through enzyme-linked immunosorbent assay (ELISA) using commercial kits, according to the manufacturer’s instructions (IL-6; BD OptEIA Human IL6 ELISA set, cat. n. 555220; TNF-α; BD OptEIA Human TNF ELISA set, cat. n. 555212, Becton & Dickinson, Franklin Lakes, USA). The AOPP was estimated by plasma levels of chloramines, which are end-products derived from protein oxidation by HOCl, the main product of neutrophil activity during inflammation, through its reaction with KI. The final reaction produces a colored compound, spectrophotometrically detected at 340 nm (Witko-Sarsat et al., 1996). Plasma concentrations of CK were determined using an automated biochemical system (Dimension EXLTM Chemistry System, Siemens, Munich, Germany).
Blood lactate concentration [Lac]
Samples of approximately 25 μl of blood were collected from the earlobe for analysis of [Lac]. Briefly, the earlobe was sanitized with alcohol 70%, and a disposable metal lancet used for puncture. Blood collection was performed using heparinized glass capillaries and the blood immediately transferred to polyethylene 1.5 ml microcentrifuge tubes containing 50 μl of sodium fluoride 1%. The tubes were stored in a container with ice, and then frozen in a freezer at −20 °C. Analysis of the [Lac] was performed using an electrochemical analyzer (YSI 2300 STAT PLUS; Copyright © Yellow Springs, Ohio, USA), with a measurement error of ± 2 %.
Data analysis
No outliers were identified using the z-score (z = (sample-mean) / standard deviation; outliers = z > 3). The Shapiro-Wilk test was used to verify data normality. Paired Student´s t tests were used to compare mean HR, %HRmax, and [Lac] between the LED and Placebo conditions. The results at pre and post moments are presented as mean ± standard deviation. A two-factor (time and group) generalized estimating equation technique (GEE) was performed for between, within, and interaction comparisons. When effects were found, a pairwise comparison with Bonferroni adjustment was performed. The ICC was used to verify the reproducibility of the HR and [Lac] measured at the first and second execution of the FISP. The ICC was interpreted using the following thresholds: .1 to .29 small, .30 to .49 moderate, .50 to .69 large, .70 to .89 very large, and .90 to 1, nearly perfect (Hopkins, 2002). All analyses were performed using IBM® SPSS® for windows version 20.0. The significance level adopted was p < .05.
Table 2
Means of Heart rate (HR), percentage of maximal heart rate (%HRmax), and Lactate concentration [Lac] of four blocks/stages of FISP
on first and second performance days and in LED and Placebo conditions.

Results
Players presented an HRmax of 194 ± 5 b.min-1 in the YO-YOIR1 test. Mean HR and %HRmax (n = 7; Table 2) were similar in both FISPs, analyzed independent of treatment performed (p = .31; p = .30 respectively), and when LED and Placebo were compared (p = .58; p = .61 respectively). Three participants were not included in the HR analyses due to technical errors associated with the HR recording. Mean [Lac] obtained in the FISP (Table 2) was similar in the first and second bouts, analyzed independent of treatment performed (p = .61), and when LED and Placebo were compared (p = .86). The ICC of HR was very large and of [Lac] nearly perfect (Figure 2).
For CMJ and IL-6, the GEE did not demonstrate interaction or group effects (p > .05), but did show an effect for time (p < .01; Table 3). The pairwise comparisons showed that CMJ presented lower values at post (p < .01) and 24h post (p = .01) compared to the pre moment and that the values at post were not different to 24h (p = 1). IL-6 blood concentration increased at post compared to pre (p < .01) and the value of IL-6 at 24h was lower than at post (p = .04) but not different from pre (p = 1), suggesting that IL-6 returned to pre values 24h post FISP. For CK, the GEE showed interaction and time effects, but did not demonstrate an effect for group (Table 3). The pairwise comparisons showed that CK increased in both Placebo (p < .01) and LED (p < .01) at the post moment compared to pre. However, no differences were found in either group when 24h was compared with pre and post moments (p > .05). For Muscle soreness, TNF-α, and AOPP, the GEE did not demonstrate interaction, time, or group effects (p > .05; Table 3).
Table 3
Values and between, within, and interaction comparisons of countermovement jump (CMJ), perceived muscle soreness, creatine kinase (CK), interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and advanced oxidation protein products (AOPP) of Placebo and LED groups at pre, post, and 24h.
Discussion
The hypothesis raised in the present study was that LED therapy could attenuate the worsening in markers of physical performance, muscle damage, inflammation, and oxidative stress of futsal players up to 24h post FISP. It is important to highlight that in contrast to what was expected, only CMJ worsened 24h post FISP. The principal results found were that LED therapy was effective for changing the CK behavior post FISP. However, no other positive effects were observed.
Attenuation of the increase in CK blood activity is one of the most likely positive effects of phototherapy reported in the literature (Nampo et al., 2016). In the present study, LED therapy changed the behavior of CK post FISP, corroborating with a previous study that showed attenuation of the increase in CK blood activity post and 48h post futsal matches (De Marchi et al., 2019). Although the pairwise comparisons did not show effects at 24h compared to pre or post, it is possible to note that values of CK remained increased after the Placebo, while this behavior was not shown after LED, possibly contributing to the interaction effect found. The mechanism related to the capacity of LED to reduce CK is still not clear (Nampo et al., 2016). However, it is possible that LED attenuates the ROS generated post exercise (that did not reflect in changes in AOPP) and increases the muscular ATP pool (Hayworth et al., 2010), attenuating EIMD. It is important to highlight that the increase in CK reported in the present study was lower than the elevation reported for athletes at 24-72h post-exercise (~400%) (Brancaccio et al., 2010). It is possible that the metabolic and physical demands of the FISP were not sufficient to promote elevated levels of muscle damage in well trained futsal players (De Freitas et al., 2017). In addition, there could be a limit to the intensity which the muscle tissue can stand, and this limit could be lower in poorly trained compared to well-trained subjects (Brancaccio et al., 2010). Therefore, for futsal players, the physical demands of FISP and, consequently, of futsal matches do not promote large EIMD. Another possibility could be that 24h was not sufficient time for the peak of CK release into the bloodstream (Brancaccio et al., 2010). However, some studies have shown that the peak of CK release was 24h post soccer matches (Magalhaes et al., 2010; Russell et al., 2015), suggesting that the time of data collection in the present study was sufficient to detect signs of muscle damage. Although the lack of measurements at 48 and 72h may be a limitation of this study, in practical use this is difficult due to the weekly training routines of athletes. Therefore, future studies are encouraged to test the effect of phototherapy on CK blood activity up to 72h post exercise with elevated physical and metabolic demands. Up to now, beneficial effects of phototherapy have been reported for reducing the elevation in CK in the blood of futsal players, even if only a slight increase in this variable is shown.
To our knowledge, this is the first study to investigate the effects of LED on CMJ performance of futsal players who performed simulated match efforts. Despite the effect of LED on CK, the results found did not suggest a positive effect of LED on performance in CMJ. It is important to note that a ~4-5% reduction in CMJ post and 24h post FISP, reported in the present study, was in accordance with previously reported results (De Freitas et al., 2017; Freitas et al., 2014). In contrast to the results found, a previous study reported a small beneficial effect of photobiomodulation on the CMJ performance of amateur soccer players (Dornelles et al., 2019). However, the present study was performed with professional futsal players, and it is possible that mechanisms other than the low level of muscle damage, such as central fatigue (Milioni et al., 2016), for example, could be responsible for the impaired performance observed in well-trained futsal players submitted to a common effort such as a futsal match.
Borges et al. (Borges et al., 2014) observed a positive effect of LED after exercise to attenuate the isometric muscular strength decrement in subjects submitted to an eccentric exercise protocol. In this study, the eccentric exercise protocol negatively modified markers of EIMD (i.e., perceived muscle soreness and range of motion) that were also attenuated by LED (Borges et al., 2014). In agreement, as previously reported (De Freitas et al., 2017), the FISP increased plasma concentration of CK, but did not change perceived muscle soreness, inflammation, or oxidative stress markers. These results suggest that if the FISP promotes EIMD, the level of damage is not sufficient to alter pain or the inflammatory and oxidative stress systemic markers analyzed in the present study. In other team sports, such as soccer, increases in muscle damage, and inflammatory and oxidative stress markers were observed 24h post matches (Magalhaes et al., 2010). However, the distance covered in soccer matches is higher than the distance covered in futsal matches (De Oliveira Bueno et al., 2014; Stolen et al., 2005), suggesting higher metabolic demands in soccer than futsal. Therefore, we encourage future studies investigating the effect of LED in subjects performing exercises with high metabolic demand, implicating in high levels of EIMD. Furthermore, although the invasive characteristic makes it difficult to perform frequent blood sample collections in professional athletes, this may be interesting in future studies since some markers, inflammatory and oxidative stress for example, present different times for release and removal from the blood (Brancaccio et al., 2010).
The use of FISP to test recovery methods may be advantageous since it imposes a similar effort on all subjects. In the present study, HR and %HRmax values monitored during the FISP in the LED and Placebo groups were similar. The values of these variables (HR, ~177-179 b.min-1; %HRmax, ~91-92%) were similar to those reported in previous studies during simulated and official futsal matches (Barbero-Alvarez et al., 2008; Castagna et al., 2009; De Freitas et al., 2017). These results were in accordance with [Lac], which did not present different values when LED and Placebo were compared, and the values reported in the present study (~6-6.5 mmol/L) were close to values reported previously (Castagna et al., 2009). Furthermore, HR, %HRmax, and [Lac] values were similar when the two times of execution of FISP were compared (independent of intervention methods), and the ICCs of HR and [Lac] were very large and nearly perfect respectively. These results may confirm that players were submitted to similar physical efforts during the two FISPs and that this was similar to the physical effort of official futsal matches.
The dose of treatment applied in the present study was in accordance with previous systematic reviews, which suggested a positive effect of phototherapy (Leal-Junior et al., 2015; Vanin et al., 2018). However, an update on the therapeutic window for large muscle groups, suggesting a large recommended dose, was published after the data collection in the present study (Leal-Junior et al., 2019). Therefore, the dose response dependence of the LED effect (Leal-Junior et al., 2015) could be a possible explanation for the limited effect found for this treatment. On the other hand, in the present study LED therapy promoted an effect on CK, suggesting that for this variable, the dose applied was effective. Whether high doses of LED are necessary to change physical performance, muscle soreness, and inflammatory and oxidative markers, should be investigated in future studies. We believe that the principal results found were a consequence of the low level of muscle damage induced by the FISP in well trained futsal players.
The number of participants could be a possible limiting factor for the results found in the present study. Unfortunately, the number of players in a futsal team is limited, and it is difficult to recruit players from different teams because of the training routines and schedules of each team. It is important to highlight that a lower sample size was used previously to show the muscle protective effect of phototherapy performed before futsal matches (De Marchi et al., 2019). However, we assume that for better understanding of the results found in the present study a large sample size may be necessary, and, thus, the sample size should be defined in future investigations. Some other points were controlled to reduce the risk of bias in the present study, such as randomization of the participants into the two groups, blinding of the participants, the presence of the Placebo, and the cross-over design of the study, factors that should be considered in the interpretation of the results found.
Conclusion
In conclusion, LED therapy applied in the present study was effective for changing CK behavior, but did not change markers of physical performance, muscle soreness, inflammation, or oxidative stress of futsal players up to 24h post FISP. It seems that the use of LED as a recovery method in well-trained futsal players post-match presented limited effects, since, apparently, for these players, a futsal effort does not promote important increases in markers associated with EIMD. In view of the positive effects reported previously, the effect of phototherapy could be more pronounced with a different dose, different sample, different level of trainability, different measurement moments, and in matches performed on consecutive days, which should be tested in future studies.
Acknowledgements
We would like to thank Prof. Fábio Yuzo Nakamura for all intellectual contribution. We would like to thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, CAPES, for providing funding for this study.
References
[1] Bangsbo, J., Iaia, F. M., & Krustrup, P. (2008). The Yo-Yo intermittent recovery test: a useful tool for evaluation of physical performance in intermittent sports. Sports Med, 38(1), 37-51. https://doi.org/10.2165/00007256-200838010-00004
[2] Barbero-Alvarez, J. C., Soto, V. M., Barbero-Alvarez, V., & Granda-Vera, J. (2008). Match analysis and heart rate of futsal players during competition. J Sports Sci, 26(1), 63-73. https://doi.org/10.1080/02640410701287289
[3] Borges, L. S., Cerqueira, M. S., Dos Santos Rocha, J. A., Conrado, L. A., Machado, M., Pereira, R., & Pinto Neto, O. (2014). Light-emitting diode phototherapy improves muscle recovery after a damaging exercise. Lasers Med Sci, 29(3), 1139-1144. https://doi.org/10.1007/s10103-013-1486-z
[4] Brancaccio, P., Lippi, G., & Maffulli, N. (2010). Biochemical markers of muscular damage. Clin Chem Lab Med, 48(6), 757-767. https://doi.org/10.1515/CCLM.2010.179
[5] Castagna, C., D’Ottavio, S., Granda Vera, J., & Barbero-Alvarez, J. C. (2009). Match demands of professional Futsal: a case study. J Sci Med Sport, 12(4), 490-494. https://doi.org/10.1016/j.jsams.2008.02.001
[6] Cook, D. B., O’Connor, P. J., Oliver, S. E., & Lee, Y. (1998). Sex differences in naturally occurring leg muscle pain and exertion during maximal cycle ergometry. Int J Neurosci, 95(3-4), 183-202. https://doi.org/10.3109/00207459809003340
[7] Dal Pupo, J., Detanico, D., & Santos, S. G. (2014). The fatigue effect of a simulated futsal match protocol on isokinetic knee torque production. Sports Biomech, 13(4), 332-340. https://doi.org/10.1080/14763141.2014.981202
[8] De Freitas, V. H., Ramos, S. P., Leicht, A., Alves, T., Rabelo, F., Bara-Filho, M. G., Guarnier, F. A., & Nakamura, F. Y. (2017). Validation of the futsal-specific intermittent shuttle protocol for the simulation of the physical demands of futsal match-play. International Journal of Performance Analysis in Sport, 17(6), 1-14. https://doi.org/10.1080/24748668.2017.1409499
[9] De Marchi, T., Leal-Junior, E. C. P., Lando, K. C., Cimadon, F., Vanin, A. A., Da Rosa, D. P., & Salvador, M. (2019). Photobiomodulation therapy before futsal matches improves the staying time of athletes in the court and accelerates post-exercise recovery. Lasers Med Sci,34(1), 139-148. https://doi.org/10.1007/s10103-018-2643-1
[10] De Moura, N. R., Cury-Boaventura, M. F., Santos, V. C., Levada-Pires, A. C., Bortolon, J., Fiamoncini, J., Pithon-Curi, T. C., Curi, R., & Hatanaka, E. (2012). Inflammatory response and neutrophil functions in players after a futsal match. J Strength Cond Res, 26(9), 2507-2514. https://doi.org/10.1519/JSC.0b013e31823f29b5
[11] De Oliveira Bueno, M. J., Caetano, F. G., Pereira, T. J., De Souza, N. M., Moreira, G. D., Nakamura, F. Y., Cunha, S. A., & Moura, F. A. (2014). Analysis of the distance covered by Brazilian professional futsal players during official matches. Sports Biomech, 13(3), 230-240. https://doi.org/10.1080/14763141.2014.958872
[12] Dornelles, M. P., Fritsch, C. G., Sonda, F. C., Johnson, D. S., Leal-Junior, E. C. P., Vaz, M. A., & Baroni, B. M. (2019). Photobiomodulation therapy as a tool to prevent hamstring strain injuries by reducing soccer-induced fatigue on hamstring muscles. Lasers Med Sci, 34(6), 1177-1184. https://doi.org/10.1007/s10103-018-02709-w
[13] Freitas, V. H., De Souza, E. A., Oliveira, R. S., Pereira, L. A., & Nakamura, F. Y. (2014). Effect of four successive days of games in muscle power, perceived stress and recovery in futsal players. Rev Bras Educ Fís Esporte, 28(1), 23-30. https://doi.org/10.1590/S1807-55092014005000002
[14] Hayworth, C. R., Rojas, J. C., Padilla, E., Holmes, G. M., Sheridan, E. C., & Gonzalez-Lima, F. (2010). In vivo low-level light therapy increases cytochrome oxidase in skeletal muscle. Photochem Photobiol, 86(3), 673-680. https://doi.org/10.1111/j.1751-1097.2010.00732.x
[15] Hopkins, W. G. (2002). A Scale of Magnitudes for Effect Statistics. https://www.sportsci.org/resource/stats/effectmag.html
[16] Leal-Junior, E. C., Vanin, A. A., Miranda, E. F., de Carvalho Pde, T., Dal Corso, S., & Bjordal, J. M. (2015). Effect of phototherapy (low-level laser therapy and light-emitting diode therapy) on exercise performance and markers of exercise recovery: a systematic review with meta-analysis. Lasers Med Sci, 30(2), 925-939. https://doi.org/10.1007/s10103-013-1465-4
[17] Leal-Junior, E. C. P., Lopes-Martins, R. A. B., & Bjordal, J. M. (2019). Clinical and scientific recommendations for the use of photobiomodulation therapy in exercise performance enhancement and post-exercise recovery: current evidence and future directions. Braz J Phys Ther, 23(1), 71-75. https://doi.org/10.1016/j.bjpt.2018.12.002
[18] Magalhaes, J., Rebelo, A., Oliveira, E., Silva, J. R., Marques, F., & Ascensao, A. (2010). Impact of Loughborough Intermittent Shuttle Test versus soccer match on physiological, biochemical and neuromuscular parameters. Eur J Appl Physiol, 108(1), 39-48. https://doi.org/10.1007/s00421-009-1161-z
[19] Milioni, F., Vieira, L. H., Barbieri, R. A., Zagatto, A. M., Nordsborg, N. B., Barbieri, F. A., Dos-Santos, J. W., Santiago, P. R., & Papoti, M. (2016). Futsal Match-Related Fatigue Affects Running Performance and Neuromuscular Parameters but Not Finishing Kick Speed or Accuracy. Front Physiol, 7, 518. doi.org/10.3389/fphys.2016.00518
[20] Nampo, F. K., Cavalheri, V., Ramos, S. P., & Camargo, E. A. (2016). Effect of low-level phototherapy on delayed onset muscle soreness: a systematic review and meta-analysis. Lasers Med Sci, 31(1), 165-177. https://doi.org/10.1007/s10103-015-1832-4
[21] Naser, N., Ali, A., & Macadam, P. (2017). Physical and Physiological demands of futsal. In Journal of Exercise Science and Fitness (Vol. 15, Issue 2, pp. 76-80). Elsevier (Singapore) Pte Ltd. http://doi.org/10.1016/j.jesf.2017.09.001
[22] Russell, M., Northeast, J., Atkinson, G., Shearer, D. A., Sparkes, W., Cook, C. J., & Kilduff, L. P. (2015). Between-Match Variability of Peak Power Output and Creatine Kinase Responses to Soccer Match-Play. J Strength Cond Res, 29(8), 2079-2085. doi.org/10.1519/JSC.0000000000000852
[23] Sattler, T., Sekulic, D., Hadzic, V., Uljevic, O., & Dervisevic, E. (2012). Vertical jumping tests in volleyball: reliability, validity, and playing-position specifics. J Strength Cond Res, 26(6), 1532-1538. https://doi.org/10.1519/JSC.0b013e318234e838
[24] Stolen, T., Chamari, K., Castagna, C., & Wisloff, U. (2005). Physiology of soccer: an update. Sports Med, 35(6), 501-536. https://doi.org/10.2165/00007256-200535060-00004
[25] Vanin, A. A., Verhagen, E., Barboza, S. D., Costa, L. O. P., &Leal-Junior, E. C. P. (2018). Photobiomodulation therapy for the improvement of muscular performance and reduction of muscular fatigue associated with exercise in healthy people: a systematic review and meta-analysis. Lasers Med Sci, 33(1), 181-214. https://doi.org/10.1007/s10103-017-2368-6
[26] Witko-Sarsat, V., Friedlander, M., Capeillere-Blandin, C., Nguyen-Khoa, T., Nguyen, A. T., Zingraff, J., Jungers, P., & Descamps-Latscha, B. (1996). Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int, 49(5), 1304-1313. https://doi.org/10.1038/ki.1996.186
ISSN: 2014-0983
Received: August 6, 2020
Accepted: April 30, 2021
Published: October 1, 2021
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


