Epidemiology and Risk Factors in Young Female Athletes: Basketball, Football, and Volleyball
Javier Peña
Beatriz Gil-Puga
Aitor Piedra
Albert Altarriba-Bartés
Eduard Loscos-Fàbregas
Iván Chulvi-Medrano
Martí Casals
Antonio García de Alcaraz
*Corresponding author: Javier Peña javier.pena@uvic.cat
Cite this article
Peña, J., Gil-Puga, B., Piedra, A., Altarriba-Bartés, A., Loscos-Fàbregas, E., Chulvi-Medrano, I., Casals, M. & García de Alcaraz, A. (2023). Epidemiology and risk factors in young female athletes: basketball, soccer, and volleyball. Apunts Educación Física y Deportes, 152, 1-12. https://doi.org/10.5672/apunts.2014-0983.es.(2023/2).152.01
Abstract
The aims of the study were to determine the epidemiological profile of young female athletes in Catalonia (Spain) who play team sports, and to analyse the risk factors for these injuries. A total of 1,235 adolescents (15 ± 2.4 years old) belonging to 168 teams from 17 clubs (n = 8 basketball, n = 3 football, and n = 6 volleyball) participated in the study. A descriptive and retrospective design was established, analysing the percentage and incidence rate of injuries, type of injury, body area, diagnosis, severity, mechanism and the context in which the injury was sustained. A binary logistic regression model was applied (p <.05) to determine relationships between factors, sports and injuries. The results indicated a higher percentage of female players injured in basketball and football, with acute, lower limb, long-term injuries that occurred without contact and in training, being more frequent. Volleyball was the sport with the lowest risk of injury, although the risk of injury increases if a second sport is not played. These findings serve to establish strategies that adapt the sporting environment to the development and characteristics of young athletes, encouraging their participation and ensuring the health of participants.
Introduction
Sports injuries are a serious public health problem (Finch & Cassell, 2006) which generates high medical costs (Sethi et al., 2008), significant psychosocial implications (Haraldsdottir & Watson, 2021), and can also be a very important determinant of citizens’ future participation in sport and physical exercise. Injuries not only affect adult athletes, but there is also a growing problem relating to sports injuries in young people. In the United States of America (USA), it has been estimated that of the 7.2 million young people who participate annually in under-18 sports competitions, approximately 2 million are injured each season, resulting in 500,000 medical service visits and 30,000 hospitalisations annually (Patel et al., 2017).
The study of the physical and physiological differences between adult and young athletes is of particular interest in understanding the occurrence of sports injuries at an early age. Such differences may make young athletes more vulnerable to health problems related to the demands of sport. Young athletes have more growth plates which are less protected against mechanical stress (Adirim & Cheng, 2003) and often use protective equipment that is inappropriate for their size, which contributes to this lack of protection. Of particular interest is compressive mechanical stress, whereby, according to the Hueter-Wolkman law, a moderate compressive load will promote growth and, on the other hand, excessive loads can damage this structure and slow or stop growth (Shapiro & Forriol, 2005). Various specialists have in the past pointed out elements such as growth spurts (which are associated with a higher risk of injury due to greater muscle-tendon stiffness and lower functional physio unit resistance), biological maturation, body measurements, training quality, inadequate pre-season training, low fitness levels, low cardiorespiratory endurance, low muscular strength level (Faigenbaum & Myer, 2010), and poor balance as intrinsic and extrinsic risk factors for injury in children and adolescents (Caine et al., 2008; Costa e Silva et al., 2022; Theisen et al., 2014). In addition, young individuals have a greater body surface area to total mass ratio, potentially leading to greater heat and fluid loss, which increases risk of dehydration and muscle injury.
Among these risk factors, those relating to gender are particularly relevant to the occurrence of injury. Generally speaking, men are more likely to experience traumatic injuries, while women are more likely to suffer injuries that will require restorative surgery (Ukogu et al., 2017). It has been highlighted through longitudinal studies that young female athletes present higher rates of overuse or repetitive mechanism injury during developmental stages (Schroeder et al., 2015). Female athletes generally suffer more hip, lower leg and shoulder injuries than male athletes, although this is highly dependent on the sporting discipline (Ristolainen et al., 2009). In addition, the influence of hormones, neuromuscular control, biomechanics, anatomy and social differences in sporting participation are some gender-related variables that result in a greater occurrence of sports injuries in female athletes (Lin et al., 2018).
In addition to the above, the role of early sports specialisation and its influence on the occurrence of sports injuries is another issue that has been widely debated in the scientific literature in recent years. Thus, young people who train in a single discipline more hours per week than their age (a ten-year-old training 11 hours per week, for example), or those who spend twice as many hours on a single discipline than in free play, are significantly more likely to be injured (Jayanthi et al., 2020). In this regard, it has been shown that specialising in a single sport increases the relative risk of patellofemoral syndrome 1.5 times, and diagnoses such as Sinding-Larsen-Johansson syndrome, patellar tendinopathy and Osgood-Schlatter disease have a four times higher relative risk in athletes who play a single sport compared to those who engage in multi-sport activity (Hall et al., 2015).
Looking more closely at team sports, a higher frequency of knee injuries (73.9%), patellofemoral dysfunction (31.3%), Osgood-Schlatter disease (10.4%), patellar tendinosis and Sinding-Larsen-Johansson syndrome (9%) was observed in young USA athletes who played basketball, volleyball and football over three seasons (Barber Foss et al., 2014). Similar results (35% knee and 21% lower back injuries) can be observed in Finnish female basketball and floorball players aged 12-20 years, also measured over three seasons. Furthermore, 44% of the recorded injuries were classified as severe (more than 28 days off training), and the occurrence of injuries was significantly higher in female players (incidence rate of 1.58 compared to male athletes of the same age and sport) (Leppänen et al., 2017).
In addition to frequency, the context in which the injury occurred is relevant. Thus, it has been observed that injury rate in competition is higher than in training for all injuries (incidence rate ratio 1.19). Similarly, female athletes with a previous musculoskeletal injury presented a higher rate of injury resulting in loss of activity than injury that does not result in a loss of activity, according to a study conducted in adolescent volleyball in the USA (McGuine et al., 2020).
Understanding the epidemiology and risk factors of each sport is key to establishing efficient strategies to prevent/reduce the risk of sports injuries (Bahr & Krosshaug, 2005). Although there are not yet many randomised control trials comparing the efficacy of modality-specific injury prevention protocols (Mugele et al., 2018), from a conceptual point of view it seems a desirable strategy, as these protocols may not only decrease the risk of injury, but may also improve discipline performance (De Hoyo et al., 2015). In this country there are few epidemiological studies similar to those described above. In this sense, using a sample of 297 athletes from across 25 sporting disciplines, Pujals et al. (2016) reveal an overall exposure injury rate (training and competition) of 4.1 injuries/1,000 hours, with an increase in injury rate corresponding to increase in competitive level. There is also a higher percentage of lower limb injuries compared to other anatomical areas, with only 21.5% of participants not suffering any sports injury in the period in which the data was collected. There were no gender differences in the occurrence of injuries, but there were differences in the ages at which injuries were sustained. Finally, there is a higher frequency and severity of injuries in cooperative-opposition sports than in individual sports. Another more recent study, comprising 498 athletes aged 14-21 years, reveals an injury incidence of 44.4%, with an average rate of 2.64 injuries/1,000 hours. The ankle (36.12%), knee (19.32%) and shoulder (6.47%) regions account for the highest number of injuries. 59.8% of the injuries occurred in training and 40.72% during competition. Likewise, the risk factors that account for a greater risk of sustaining an injury were: more hours of practice per week, not warming up, using inadequate sports facilities, being between 14 and 17 years old, and not doing physical training (Prieto-González et al., 2021).
For all of the above reasons, it is of scientific and social interest to study the specific epidemiology and risk factors in young female athletes participating in team sports. Therefore, the objectives of the present study were: (i) to determine the specific epidemiological profile of young female team sports athletes in Catalonia (Spain), (ii) to analyse the risk factors for these injuries, (iii) to provide information for developing more effective and specific injury prevention protocols for each sport.
Methodology
A total of 1,439 female athletes (15 ± 2.4 years; range 11-21) belonging to 168 teams from 17 basketball (n = 8), football (n = 3) and volleyball (n = 6) clubs were the subject of the study. Based on data from the sports federations to which hey are affiliated, a purposive sample determined the sports teams that were selected for participation in the study, using their sporting level as the inclusion criterion (Table 1). Those who responded positively to an invitation participated. Thus, data from 1,235 players (85.8%) were included in the final analysis. The 204 players (14.2%) who were excluded from the analysis did not meet the inclusion criteria (Table 1), were not available on the day of data collection at their club, or did not want to participate in the study.
Statistical power
The total number of federation licences for these three sports in Catalonia (Spain) for female athletes in the 2018-2019 season was 35,352, according to data provided by the corresponding federations. The sample collected in this study represents 3.5% of the total number of participants in these sports. This sample size allows population values to be inferred with 95% confidence and 4% precision, using an expected injury ratio of .56 (56%). This ratio was determined using previous studies with participants exhibiting similar characteristics (Eapen, 2014; Owoeye et al., 2020).
Materials and Resources
The data collection process for the present research was conducted through a retrospective observational study conducted between September 2019 and March 2020, which collected data from the 2018-2019 season provided by the athletes themselves and/or their legal guardians using a collection instrument based on the Orchard Sports Injury Classification System (OSICS) Version 10 (Rae & Orchard, 2007) and the International Olympic Committee recommendations for monitoring sports injuries in multi-sport events (Junge et al., 2008). Only injuries requiring medical attention were considered in this study (Timpka et al., 2014). The questionnaire, in its updated format, is available on demand on the SONAR project website: www.sonarinjuries.com. All data were collected by two of the researchers (BG-P and EL-F) after a period of training in use of the instrument, and after first conducting a pilot study.
Statistical Analysis
Firstly, a descriptive study was carried out. Results for continuous variables were expressed as a mean, standard deviation, minimum and maximum when following a normal distribution, while qualitative or categorical variables were shown as number and percentage. Variables were compared using the χ2 test for qualitative variables, and a binary logistic regression model was used with the input method applying the criterion injury (1), non-injury (0), to look for correlations with quantitative variables. All analyses were carried out with JASP for Mac (Version 0.16.1, University of Amsterdam, The Netherlands, 2021) and statistical significance was set to p <.05. Some of the graphs presented here were produced using JASP software, and others with Microsoft Excel for Mac (Version 16.58, Microsoft Corporation, USA, 2021).
Ethical considerations
Before collecting the information via questionnaire, clubs, managers, legal guardians and athletes were informed of all study procedures. Written informed consent was obtained from all participants or their legal guardians in the case of athletes under 16 years of age. All information was collected anonymously, guaranteeing the protection of personal data and following the European directives in force at the time of the study. The procedures carried out respected the Declaration of Helsinki guidelines and its subsequent updates at all times. The Research Ethics Committee of the University of Vic-Central University of Catalonia approved the content of the study and all its procedures (favourable report with internal code 71/2019).
Results
Study participants had an average number of years of sport practice of 6.5 ± 2.8 years (minimum 1 year, maximum 16 years), an average number of years of federation sport practice of 5.1 ± 2.7 years (minimum 0 years, maximum 14 years) and an average number of hours of training per week (excluding time spent in competition) of 5.5 ± 2.4 hours/week (minimum 1 hour per week, maximum 20 hours per week). 19% of federation sportswomen did not participate in school physical education, and only 11% of sportswomen practised more than one sport in the same period.
Forty-one percent of the female athletes surveyed had some kind of injury that required medical attention. Analysis by sport showed that basketball was the sport with the highest percentage of injured players (48%), followed by football (38%) and volleyball (30%). In terms of total injuries, the highest incidence rate was observed in basketball (0.046 injuries/1,000 h), followed by volleyball (0.034 injuries/1,000 h) and football (0.030 injuries/1,000 h) (Table 2). Incidence rates were calculated using only the training hours reported by the athletes.
Table 2
Number of participants, injured players, percentage, total injuries, incidence and incidence rate by sport.
In terms of injury type, the most common was found to be those injuries that are acute/traumatic in nature (67%), followed by repetitive and gradual onset mechanism injury (17.5%), and injuries caused by several possible mechanisms (14.5%), such as anterior cruciate ligament injuries (Table 3).
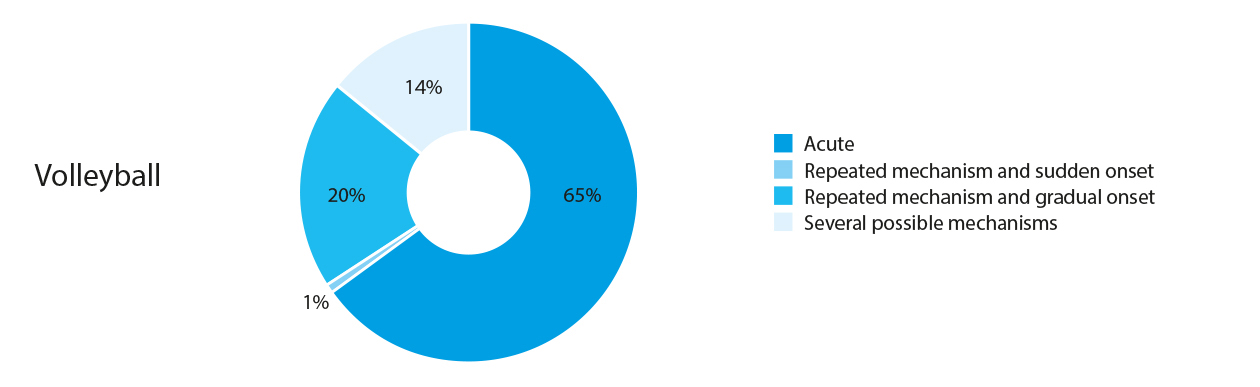
The Chi-squared test demonstrated that the observed incidence of each type of injury was not significantly different between the sports analysed (χ2= 7.879; p = .247) (Figures 1, 2 and 3).


In the study of the area of the body injured, no statistically significant differences were found between the type of injury and the dominant arm (χ2= 4.492; p = .610) or leg (χ2= 2.478; p = .871) of female athletes. The anatomical area most commonly injured in the initial injury sustained was the ankle (35%), followed by the knee (17%) and the hands or fingers (13.6%) (Figure 4), and the most common diagnosis was an ankle sprain (40%) (Figure 5).

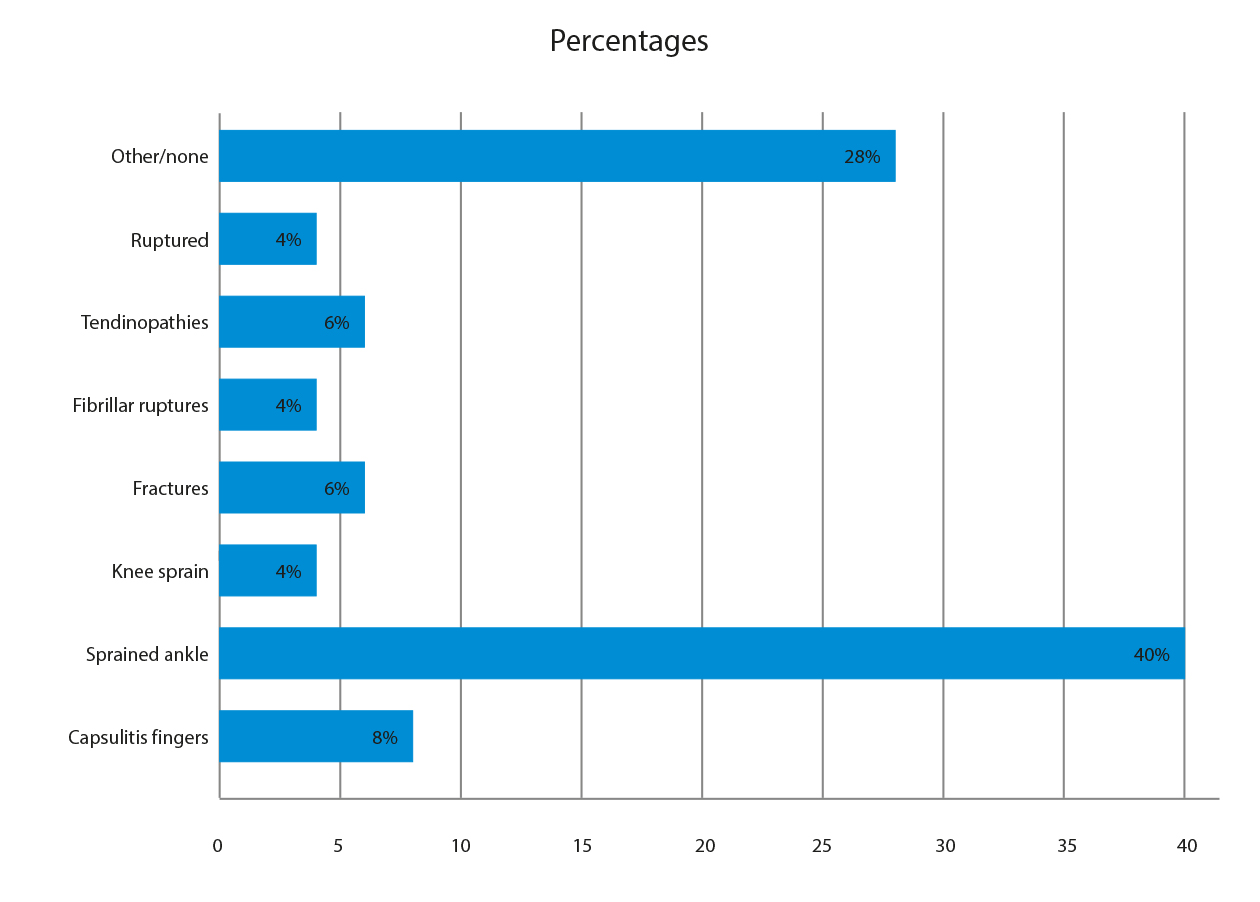
In terms of the second injury sustained in the same season (12% of the athletes), the most commonly injured anatomical area was again the ankle (36.5%), followed by the hands/fingers (15.5%) and the knee (14.1%). The most frequent diagnosis for second injuries was an ankle sprain (38%), fractures (12%) and capsulitis of the toes (11%). Only 2.2% of second injuries recorded (n = 28) were recurrent injuries that had already been sustained that season or even in previous seasons.
Regarding the diagnoses of all injuries, and comparing the different sporting disciplines (Table 4), it was observed that basketball and football had a higher percentage of ankle sprains (34% in both cases), as well as more fractures (7% and 8%, respectively). Football had a higher percentage of knee ligament tears (5%), while tendinopathies (10%) and toe capsulitis (9%) were more frequent in volleyball.
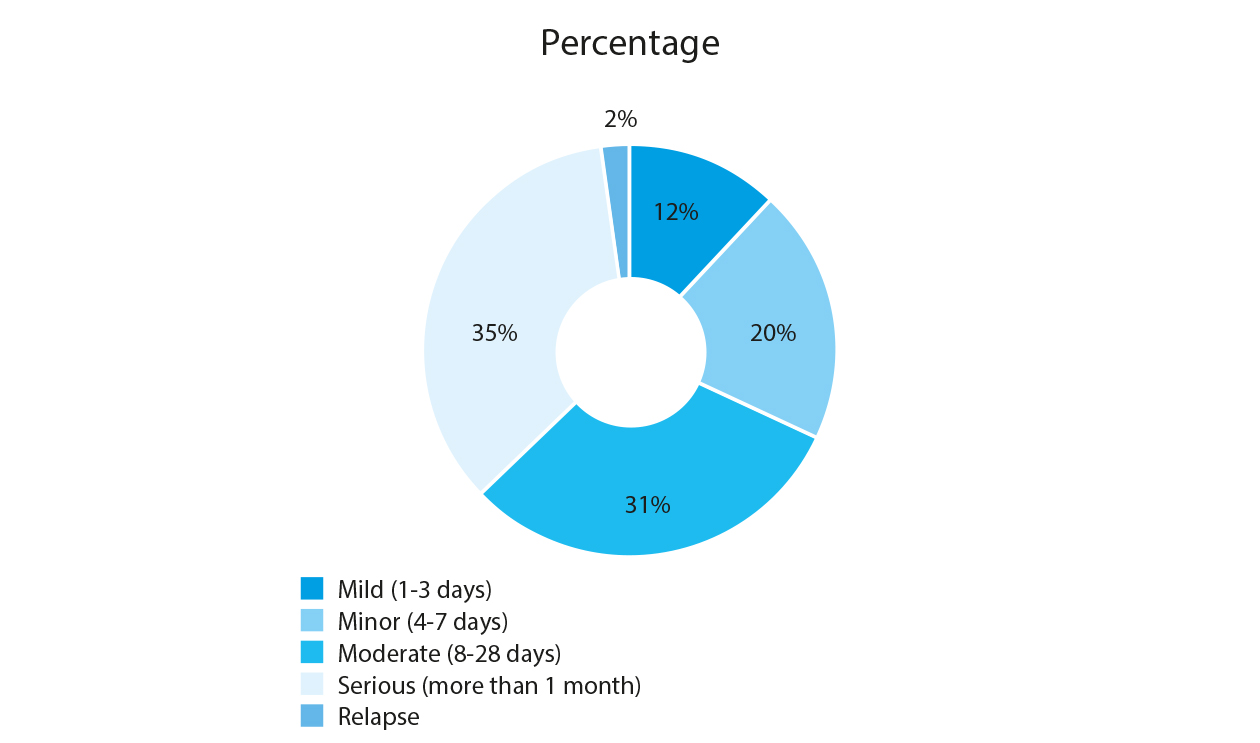
Figure 6 shows the percentage of injuries classified by severity. Of the total number of injuries, 31% were moderate (8-28 days) and, as mentioned above, only 2% of the total number of injuries were recurrent or relapsing injuries.
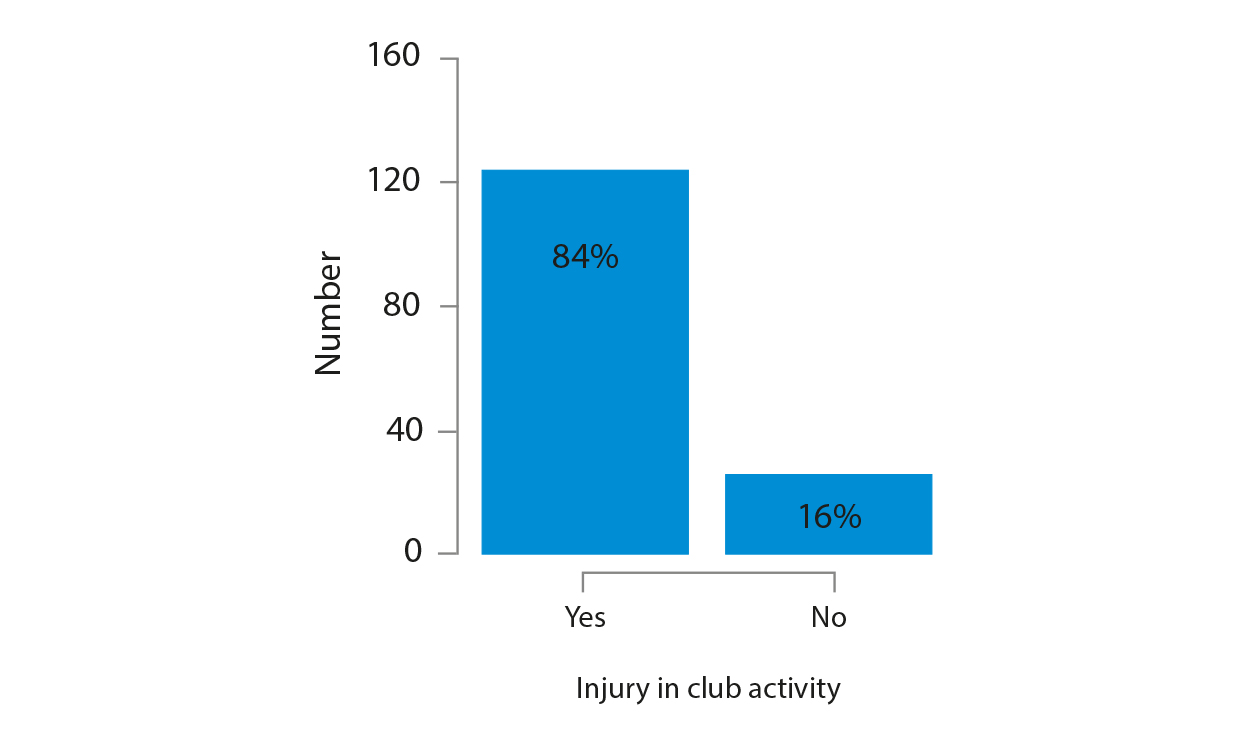
The majority of reported injuries occurred without contact (43%), in training (51%), and in club activity (85%), as depicted in figures 7, 8 and 9 (Figures 7, 8 and 9).


A binary logistic regression test was conducted to determine the effects of age, preferred sport, years of playing that sport, years of playing that sport as a federation sport, hours of practice per week, playing a second sport, hours spent playing a second sport, whether or not the sport was part of school physical education and hours of physical education, on the likelihood of participants sustaining a sports injury. The logistic regression model was statistically significant (χ2 (1,217) = 49.902; p <.001), revealing a sensitivity of 21% and a specificity of 89.5%.
Of all the factors analysed, only volleyball was associated with a decreased risk of injury compared to the other sports (volleyball = 20%; basketball = 62%; football = 65%) (Figure 10). When playing volleyball, a connection was also found between not playing a second sport and the probability of sustaining an injury, which in this case increased 2.5 times (Table 5).

Table 5
Binary logistic regression model variables showing statistically significant association with injury occurrence.
Discussion
The main aim of this study was to determine the specific epidemiological profile of young female team sport players in Catalonia, analysing the risk factors for these injuries. The results show that the percentage of injured players is higher in basketball and football, with a higher injury incidence rate in basketball. These findings are consistent with those of García González et al. (2015), who found that the sports with the highest injury rates were football (27.6%), running (8.6%), indoor football (7.9%) and basketball (7.7%) in an epidemiological study on Spanish leisure sports.
Acute injury is the most frequent type of injury, with no significant differences between sports. Injuries to the lower limbs (ankles and knees), that are long term (more than 28 days without training), sustained without contact and in training were also the most common among young athletes. Finally, volleyball appears to be the sport with the lowest risk of injury, although the probability of injury increases if a second sport is not played.
Although in sports such as basketball and football the simultaneous occupation of space allows for some contact between players, most injuries occur without contact and acutely in all sports. The lower risk of injury associated with volleyball has traditionally been accounted for by the lack of contact between athletes, but, in view of these results, other factors could be conditioning these incidence rates (training time and competition effort, player substitutions, means of recovery, etc.). These data create a need to address the movement patterns that have caused the injury, analysing how biomechanical factors focused on the kinematics or kinetics of movement, neurophysiological aspects such as fatigue and decreased coordination capacity, or psycho-physiological variables related to the sporting context are contributing to injury.
In relation to body area, this study shows an increase in ankle injuries, compared to the predominance of knee injuries found in other studies (Leppänen et al., 2017). The explosive jumping action, which is very common in basketball and volleyball, as well as changes of direction or support on uneven surfaces in football, could explain this fact. In this sense, the high number of hand injuries reported for volleyball would be related to the hits and interceptions typical of actions of maximum intensity such as spiking and blocking, especially the latter.
Analysing the context of injury, it is surprising that the training setting is the most common in terms of number of injuries, as competitive demand, both physically and psychologically, often indicates higher injury rates in matches (McGuine et al., 2020). It is possible that the characteristics of the sample influenced these results. It could be hypothesised that the lack of homogeneity in aspects such as average number of years of sport practice, average number of years of federation sport practice, or average number of hours of training per week among the participants may have conditioned these results.
The importance of playing a second sport to reduce the risk of injury in young volleyball players could be related to the importance of different movements in order to avoid repetitive patterns that can lead to overuse injuries, or acute injuries at a predetermined sporting instant. This is consistent with multi-sport development approaches, which appreciate that a wide range of experiences based on the practice of numerous sporting activities improves participation in a sport, while increasing the likelihood of success and decreasing the risk of injury (Carder et al., 2020). And, although analysis of the reasons for the reduction of injury risk is beyond the scope of this review, it is worth highlighting that the practice of various sporting disciplines will allow young athletes to increase their motor literacy and, with it, the control of various movement challenges for motor control (DiStefano et al., 2018). This recommendation is applicable in all contexts, although in this study we only found an association between the likelihood of a lower risk of injury when playing another sport in volleyball players.
It should be noted that none of the 7 injuries recorded as being located on the face/head were diagnosed as concussion. This suggests that in Catalonia this condition may still be under-reported in medical settings, as in other scientific evidence Ia studies (Pfister et al., 2016) the incidence stands at 0.23 injuries per 1,000 h of exposure in football, 0.13 in basketball and 0.03 in volleyball. This fact requires special focus since, although it has been reported in other sports, such as judo, head injuries can be a clear risk factor for triggering acute subdural haemorrhage (Nagahiro & Mizobuchi, 2014). Also, the risk of repeated head trauma can trigger long-term fatal effects, such as encephalopathies (Cantu & Bernick, 2020). Therefore, the importance of paying attention to face/head injuries in order to prevent negative effects is justified.
In Spain there is currently no national programme for monitoring sporting injuries. In fact, care for this sport-related health problem is fragmented between the private sector (hospitals and sports mutual insurance companies) and the public health system. This situation, as well as the current European regulations on personal data protection, makes it very difficult for initiatives to publicise in detail the extent of the problem of sporting injuries in children and adolescents. Therefore, scientific studies revealing epidemiological data and assessing risk factors are needed in order to implement age-, gender- and sport-specific prevention strategies, as well as policies or changes in sporting regulations aimed at improving the health of young athletes.
Conclusions
The results obtained in relation to the epidemiological profile of young sportsmen and women in Catalonia indicate that a higher percentage of injuries occur in basketball and football, with volleyball being the sport with the least injuries. Acute injuries are the most common injuries in all sports, as well as lower limb injuries occurring without contact and in training situations. Most of the injuries resulted in long-term absences. The practice of a second sport at this age is also recommended to reduce the risk of injury, especially in volleyball. These findings could be useful for helping coaches, physical trainers and sport managers, as well as the athletes themselves, establishing injury prevention programmes adapted to the sport practiced, preparing athletes in a way that is consistent with their development, and generating regulations and competition environments adapted to the characteristics of young female athletes. Furthermore, it opens up an interesting line of research into examining the mechanisms of injury, preventing an increase in incidence rate and encouraging participation in sports programmes in this age group and gender.
Limitations
The present study is observational and retrospective (evidence IIb), and does not allow cause-effect relationships to be established. The information was collected from the players themselves, which results in the loss of some diagnoses, as well as giving rise to inaccuracies in some answers due to memory bias, despite the fact that the collection procedure was conducted rigorously. The participating clubs were selected through purposive sampling, so there is a selection bias in this study despite its large sample size. The injury incidence rate for each of the disciplines was calculated using training hours only. As we are talking about very different disciplines, with very different match times in competition, and as we did not have any reliable instrument for recording the playing time of each player, it was impossible to incorporate this information in the final calculation. In some cases, two mechanisms of injury are possible and the analysis of injury mechanisms has considered four possibilities instead of the usual three. In addition, there was a great deal of heterogeneity in the professionals who diagnosed them. Finally, the sample was uneven for each sport, preventing balanced comparisons in all cases.
Acknowledgements
We would like to thank all the sportswomen, mothers, fathers, clubs and sporting clubs that participated in the study, altruistically providing information that can contribute to improving the health of other sportswomen in the future.
Funding
This study is part of the SONAR project “Epidemiological study of competitive sport injuries in young athletes” of the University of Vic-Central University of Catalonia, funded through a knowledge transfer contract (reference 794/U013/1) with the College of Physical Activity and Sport Professionals of Catalonia (COPLEFC).
References
[1] Adirim, T. A. & Cheng, T. L. (2003). Overview of injuries in the young athlete. Sports Medicine, 33(1), 75–81. https://doi.org/10.2165/00007256-200333010-00006
[2] Bahr, R. & Krosshaug, T. (2005). Understanding injury mechanisms: a key component of preventing injuries in sport. British Journal of Sports Medicine, 39(6), 324–329. https://doi.org/10.1136/bjsm.2005.018341
[3] Barber Foss, K. D., Myer, G. D. & Hewett, T. E. (2014). Epidemiology of basketball, soccer, and volleyball injuries in middle-school female athletes. Physician and Sportsmedicine,42(2), 146–153. https://doi.org/10.3810/psm.2014.05.2066
[4] Caine, D., Maffulli, N. & Caine, C. (2008). Epidemiology of Injury in Child and Adolescent Sports: Injury Rates, Risk Factors, and Prevention. Clinics in Sports Medicine, 27(1), 19–50. https://doi.org/10.1016/j.csm.2007.10.008
[5] Cantu, R. C. & Bernick, C. (2020). History of Chronic Traumatic Encephalopathy. Seminars in Neurology, 40(04), 353–358. https://doi.org/10.1055/s-0040-1713622
[6] Carder, S. L., Giusti, N. E., Vopat, L. M., Tarakemeh, A., Baker, J., Vopat, B. G. & Mulcahey, M. K. (2020). The Concept of Sport Sampling Versus Sport Specialization: Preventing Youth Athlete Injury: A Systematic Review and Meta-analysis. The American Journal of Sports Medicine, 48(11), 2850–2857. https://doi.org/10.1177/0363546519899380
[7] Costa e Silva, L., Teles, J. & Fragoso, I. (2022). Sports injuries patterns in children and adolescents according to their sports participation level, age and maturation. BMC Sports Science, Medicine and Rehabilitation, 14(1), 35. https://doi.org/10.1186/s13102-022-00431-3
[8] De Hoyo, M., Pozzo, M., Sañudo, B., Carrasco, L., Gonzalo-Skok, O., Domínguez-Cobo, S. & Morán-Camacho, E. (2015). Effects of a 10-Week In-Season Eccentric-Overload Training Program on Muscle-Injury Prevention and Performance in Junior Elite Soccer Players. International Journal of Sports Physiology and Performance, 10(1), 46–52. https://doi.org/10.1123/ijspp.2013-0547
[9] DiStefano, L. J., Beltz, E. M., Root, H. J., Martinez, J. C., Houghton, A., Taranto, N., Pearce, K., McConnell, E., Muscat, C., Boyle, S. & Trojian, T. H. (2018). Sport Sampling Is Associated With Improved Landing Technique in Youth Athletes. Sports Health: A Multidisciplinary Approach, 10(2), 160–168. https://doi.org/10.1177/1941738117736056
[10] Eapen, C. (2014). Prevalence of Sports Injuries in Adolescent Athletes. Journal of Athletic Enhancement, 03(05). https://doi.org/10.4172/2324-9080.1000168
[11] Faigenbaum, A. D. & Myer, G. D. (2010). Resistance training among young athletes: safety, efficacy and injury prevention effects. British Journal of Sports Medicine, 44(1), 56–63. https://doi.org/10.1136/bjsm.2009.068098
[12] Finch, C. & Cassell, E. (2006). The public health impact of injury during sport and active recreation. Journal of Science and Medicine in Sport, 9(6), 490–497. https://doi.org/10.1016/j.jsams.2006.03.002
[13] García González, C., Albaladejo Vicente, R., Villanueva Orbáiz, R. & Navarro Cabello, E. (2015). Epidemiological Study of Sports Injuries and their Consequences in Recreational Sport in Spain. Apunts Educación Física y Deportes, 119, 62–70. https://doi.org/10.5672/apunts.2014-0983.es.(2015/1).119.03
[14] Hall, R., Foss, K. B., Hewett, T. E. & Myer, G. D. (2015). Sport Specialization’s Association With an Increased Risk of Developing Anterior Knee Pain in Adolescent Female Athletes. Journal of Sport Rehabilitation, 24(1), 31–35. https://doi.org/10.1123/jsr.2013-0101
[15] Haraldsdottir, K. & Watson, A. M. (2021). Psychosocial Impacts of Sports-related Injuries in Adolescent Athletes. Current Sports Medicine Reports, 20(2), 104–108. https://doi.org/10.1249/JSR.0000000000000809
[16] Jayanthi, N., Kleithermes, S., Dugas, L., Pasulka, J., Iqbal, S. & LaBella, C. (2020). Risk of Injuries Associated With Sport Specialization and Intense Training Patterns in Young Athletes: A Longitudinal Clinical Case-Control Study. Orthopaedic Journal of Sports Medicine, 8(6), 232596712092276. https://doi.org/10.1177/2325967120922764
[17] Junge, A., Engebretsen, L., Alonso, J. M., Renstrom, P., Mountjoy, M., Aubry, M. & Dvorak, J. (2008). Injury surveillance in multi-sport events: the International Olympic Committee approach. British Journal of Sports Medicine, 42(6), 413–421. https://doi.org/10.1136/bjsm.2008.046631
[18] Leppänen, M., Pasanen, K., Kannus, P., Vasankari, T., Kujala, U., Heinonen, A. & Parkkari, J. (2017). Epidemiology of Overuse Injuries in Youth Team Sports: A 3-year Prospective Study. International Journal of Sports Medicine, 38(11), 847–856. https://doi.org/10.1055/s-0043-114864
[19] Lin, C. Y., Casey, E., Herman, D. C., Katz, N. & Tenforde, A. S. (2018). Sex Differences in Common Sports Injuries. PM&R, 10(10), 1073–1082. https://doi.org/10.1016/j.pmrj.2018.03.008
[20] McGuine, T. A., Post, E., Biese, K., Kliethermes, S., Bell, D., Watson, A., Brooks, A. & Lang, P. (2020). The Incidence and Risk Factors for Injuries in Girls Volleyball: A Prospective Study of 2072 Players. Journal of Athletic Training. https://doi.org/10.4085/182-20
[21] Mugele, H., Plummer, A., Steffen, K., Stoll, J., Mayer, F. & Müller, J. (2018). General versus sports-specific injury prevention programs in athletes: A systematic review on the effect on injury rates. PLOS ONE, 13(10), e0205635. https://doi.org/10.1371/journal.pone.0205635
[22] Nagahiro, S. & Mizobuchi, Y. (2014). Current topics in sports-related head injuries: A review. Neurologia Medico-Chirurgica, 54(11), 878–886. https://doi.org/10.2176/nmc.ra.2014-0224
[23] Owoeye, O. B. A., Ghali, B., Befus, K., Stilling, C., Hogg, A., Choi, J., Palacios‐Derflingher, L., Pasanen, K. & Emery, C. A. (2020). Epidemiology of all‐complaint injuries in youth basketball. Scandinavian Journal of Medicine & Science in Sports, 30(12), 2466–2476. https://doi.org/10.1111/sms.13813
[24] Patel, D. R., Yamasaki, A. & Brown, K. (2017). Epidemiology of sports-related musculoskeletal injuries in young athletes in United States. Translational Pediatrics, 6(3), 160–166. https://doi.org/10.21037/tp.2017.04.08
[25] Pfister, T., Pfister, K., Hagel, B., Ghali, W. A. & Ronksley, P. E. (2016). The incidence of concussion in youth sports: A systematic review and meta-analysis. British Journal of Sports Medicine, 50(5), 292–297. https://doi.org/10.1136/bjsports-2015-094978
[26] Prieto-González, P., Martínez-Castillo, J. L., Fernández-Galván, L. M., Casado, A., Soporki, S. & Sánchez-Infante, J. (2021). Epidemiology of sports-related injuries and associated risk factors in adolescent athletes: An injury surveillance. International Journal of Environmental Research and Public Health, 18(9). https://doi.org/10.3390/ijerph18094857
[27] Pujals, C., Rubio, V. J., Marquez, M. O., Sánchez, I. & Ruiz-Barquin, R. (2016). Comparative sport injury epidemiological study on a Spanish sample of 25 different sports. Revista de Psicología del Deporte, 25(2), 271–279.
[28] Rae, K. & Orchard, J. (2007). The Orchard Sports Injury Classification System (OSICS) Version 10. Clinical Journal of Sport Medicine, 17(3), 201–204. https://doi.org/10.1097/JSM.0b013e318059b536
[29] Ristolainen, L., Heinonen, A., Waller, B., Kujala, U. M. & Kettunen, J. A. (2009). Gender differences in sport injury risk and types of injuries: A retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. Journal of Sports Science and Medicine, 8(3), 443–451.
[30] Schroeder, A. N., Comstock, R. D., Collins, C. L., Everhart, J., Flanigan, D. & Best, T. M. (2015). Epidemiology of Overuse Injuries among High-School Athletes in the United States. The Journal of Pediatrics, 166(3), 600–606. https://doi.org/10.1016/j.jpeds.2014.09.037
[31] Sethi, D., Towner, E., Vincenten, J., Segui-Gomez, M. & Racioppi, F. (2008). European report on child injury prevention. https://www.sanidad.gob.es/va/profesionales/saludPublica/prevPromocion/Prevencion/SeguridadVial/docs/europeanReporChild.pdf
[32] Shapiro, F. & Forriol, F. (2005). Growth cartilage: developmental biology and biomechanics. Revista Española de Cirugía Ortopédica y Traumatología, 49(1), 55–67. https://doi.org/10.1016/S1888-4415(05)76272-X
[33] Theisen, D., Malisoux, L., Seil, R. & Urhausen, A. (2014). Injuries in Youth Sports: Epidemiology, Risk Factors and Prevention. Deutsche Zeitschrift Für Sportmedizin, 2014(09), 248–252. https://doi.org/10.5960/dzsm.2014.137
[34] Timpka, T., Jacobsson, J., Bickenbach, J., Finch, C. F., Ekberg, J. & Nordenfelt, L. (2014). What is a Sports Injury? Sports Medicine, 44(4), 423–428. https://doi.org/10.1007/s40279-014-0143-4
[35] Ukogu, C., Patterson, D., Sarosi, A. & Colvin, A. C. (2017). Epidemiology of youth sports injury: a review of demographic and sports-related risk factors for injury. Annals of Joint, 2, 79–79. https://doi.org/10.21037/aoj.2017.12.04
ISSN: 2014-0983
Received: July 5, 2022
Accepted: October 7, 2022
Published: April 1, 2023
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


