Bilateral comparison of shoulder range of motion and peak isometric strength in amateur tennis players
Roger Jové
Albert Busquets Faciabén
Neus Camins
Manuel Añón
Blai Ferrer-Uris
*Corresponding author: Blai Ferrer-Uris bferrer@gencat.cat
Cite this article
Jové, R., Busquets, A., Camins, N., Añón, M. & Ferrer-Uris, B. (2023). Bilateral comparison of shoulder range of motion and peak isometric strength in amateur tennis players. Apunts Educación Física y Deportes, 154, 108-115. https://doi.org/10.5672/apunts.2014-0983.es.(2023/4).154.10
Abstract
Lower values of shoulder internal rotation range of motion (ROM-IR) and external/internal rotation strength ratio (S-ER/S-IR) of the dominant arm (racket grip) compared to the non-dominant arm have been observed in professional tennis players. It is considered that these adaptations could increase the risk of shoulder injury. Little is known about these adaptations in amateur tennis players. The aim of this study was to bilaterally compare the range of motion (ROM) and peak isometric strength (S) of shoulder rotation movements in amateur tennis players (dominant arm [DA] versus non-dominant arm [NDA]). In thirteen amateur tennis players (18-45 years old) the passive ROM and the S of internal rotation (IR) and external rotation (ER) were measured from the supine position, 90° of shoulder abduction and 90° of elbow flexion. DA and NDA values were compared by paired samples T-test. DA had lower ROM-IR (t = –9.053; p < .001; d = –2.551) and total ROM-(t = –4.429; p < .001; d = –1.228) compared to NDA (ΔROM-IR = 23.73 %; ΔROM-total = 8.32 %). Greater DA S-IR was also detected compared to NDA (t = 2.344, p = .037, d = .650, ΔS-IR = 9.67 %). These results indicate the existence of unilateral adaptations of the shoulder, which have been identified in other publications as risk factors for injury. In contrast to observations in professional tennis players in other studies, no S-related injury risk indicators were found.
Introduction
Tennis is a sport that involves a large number of overhead arm movements. These movements occur mainly when serving and smashing. For example, all points in a match are initiated by a serve, which makes this action one of the main game actions and accounts for 45-60% of all hitting actions in the match (Johnson & McHugh, 2006). These tennis hitting actions are performed in a highly explosive manner with the aim of delivering the ball at high speeds, with records of up to 210 km/h top speed on serves at professional levels (Kovacs, 2007). In these tennis hitting actions, the shoulder is at the central point of the sequence that generates, aggregates and transmits kinetic energy from the lower limbs to the racket (Van Der Hoeven & Kibler, 2006). The highly complex and mobile anatomical characteristics of the shoulder mean that it has poorly congruent articular surfaces, thereby conferring a critical role on the adjacent ligaments and musculature for joint stability (Felstead & Ricketts, 2017). Both factors, the high number of repetitions of the hitting actions combined with the explosiveness of the movements, expose the player to a high risk of injury, especially overuse or chronic injuries (Pluim et al., 2006; Renstrom & Johnson, 1985). In fact, previous studies have shown that most chronic injuries in professional tennis occur in the upper arm and that a large proportion of these injuries occur in the shoulder joint complex (Pluim et al., 2006; Van Der Hoeven & Kibler, 2006). Moreover, the review by Abrams et al. (2012) revealed that in tennis players at all levels, not just professionals, shoulder injuries accounted for between 4 and 17% of all injuries and that the number of players reporting shoulder pain increased to 50% in middle-aged adult players. Thus, understanding the risk factors associated with shoulder injuries in tennis players is a relevant issue that can help in the design of interventions and training plans aimed at improving the performance and health of the athlete (Prieto-González & Brahim, 2018; Prieto-González & Larumbe-Zabala, 2021).
This situation of risk can be highly aggravated when there are functional deficits of the shoulder joint. Previous studies have shown how impaired range of motion and/or strength of the shoulder joint can be an important factor linked to shoulder injuries. In fact, some studies (Ellenbecker, 1992; Kibler et al., 1996) have observed that in high-level tennis players there are several alterations related to the range of motion and strength of the internal rotation (IR) and external rotation (ER) movements of the racquet grip arm or dominant arm (DA). In the review by Pluim et al. (2006), 6 out of 7 studies reported a decrease in both the range of motion in IR (ROM-IR) and total range of motion (ROM-T) of DA shoulder rotation compared to the non-dominant arm (NDA). Furthermore, Kibler et al. (1996) demonstrated how the differences between DA and NDA in range of motion worsened with years of experience in high-level players. This same trend has been observed in other sports involving overhead hitting and throwing actions, which show a high prevalence of decreased ROM-IR and ROM-T of DA versus NDA (Hams et al., 2019). Furthermore, these reductions in ROM have been used as a predictor of shoulder injuries (Corbi & Baiget, 2015; Hams et al., 2019). In relation to strength, the review by Pluim et al. (2006) showed that in 5 studies (out of 7) the IR strength (S-IR) was higher in the DA than in the NDA. This increase in S-IR also implied a lower strength ratio between the ER and IR (S-ER/S-IR ratio) of the DA compared to the NDA. It has been proposed that an increase in S-IR that is not in balance with S-IR may be a risk factor for injury, as the external rotational musculature may not be able to decelerate and stabilise the shoulder joint at the end of ball smashing actions (Ellenbecker, 1992). It has also been estimated that a difference in rotational strength between limbs of 10-15% may increase the risk of injury (Corbi & Baiget, 2015). Thus, the presence of these alterations related to range of motion or strength in shoulder rotational movements may increase susceptibility to injury during tennis strokes. In particular, a significant risk situation could arise when both factors are present simultaneously. For example, athletes who are capable of generating large IR strength would not be able to stop the accelerations generated during smashing actions because of low levels of strength in the ER. This could mean that during the post-smash deceleration phase in the arm, the joint position could dangerously approach or exceed the maximum ROM-IR of the joint.
As a result of the above issues and the differences between DA and NDA found in the case of high level tennis players, there is a growing awareness of the importance of monitoring the range of motion and strength of both arms in order to control and reduce the risk of injury. However, the extent of this problem is not well documented outside the field of top-level tennis. More than 33,500 adult women and men play tennis at amateur level under a federation licence in Spain alone (Real Federación Española de Tenis, 2021) and invest a large number of hours per week in training and competitions. The number of amateur players is greater than the number of high-level players and, in addition, tennis is a sport played by adults of various ages. Therefore, it is necessary to study whether in adult amateur players there are alterations in terms of range of motion and strength of the dominant arm movements of IR and ER that could predispose this population to a risk of shoulder injury. Thus, the objectives of this study were as follows: (1) to evaluate the differences in IR (ROM-IR), ER (ROM-ER) and total (ROM-T) range of motion between the DA and NDA shoulder in adult amateur tennis players; and (2) to compare the IR (S-IR), ER (S-ER) strength and S-ER/S-IR ratio of the DA and NDA shoulder in adult amateur level tennis players.
Method
Participants
A total of 13 tennis players participated in the study (biological sex): 12 male, 1 female; age: 32 ± 10.8 years old; height: 1.81 ± 0.1 m; weight: 77.9 ± 10.1 kg; dominant arm: 11 right-handed, 2 left-handed; age when starting tennis: 6.8 ± 2.5 years old; hours per week: 7.6 ± 2.5 h/set). The requirements for participation in the study were: (1) being 18 years of age or older, (2) having started playing and training for tennis almost every day since childhood (5-12 years old), (3) playing tennis between 3 and 15 hours per week, and (4) being free of injury and/or discomfort in the shoulder joint for the last 6 months. The study was conducted in accordance with the Declaration of Helsinki. All participants gave written consent for participation in this study after receiving a detailed explanation of the procedures. The study was approved by the Clinical Research Ethics Committee of the Catalan Sports Administration (031-CEICGC-2022).
Procedure
At the beginning of the assessment session, participants completed a questionnaire with information regarding personal data, tennis history and shoulder health history. This questionnaire was used to assess the inclusion criteria for the study. The participants then performed two different tests: firstly, a passive range of motion (ROM) assessment test and, secondly, a peak isometric strength (S) assessment test, both applied to the internal rotation (IR) and external rotation (ER) movements of the shoulder. Prior to initiation of the two tests, all participants did a warm-up consisting of: (1) two sets of 12 repetitions of shoulder IR and ER with medium resistance rubber bands, with the shoulder positioned in 90° abduction and the elbow flexed to 90°; and (2) submaximal passive stretching of the IR and ER movements, following the same execution protocol as that used for the range of motion test. This second part of the warm-up also serves as preparation for the passive range of motion test.
Passive range of motion assessment test
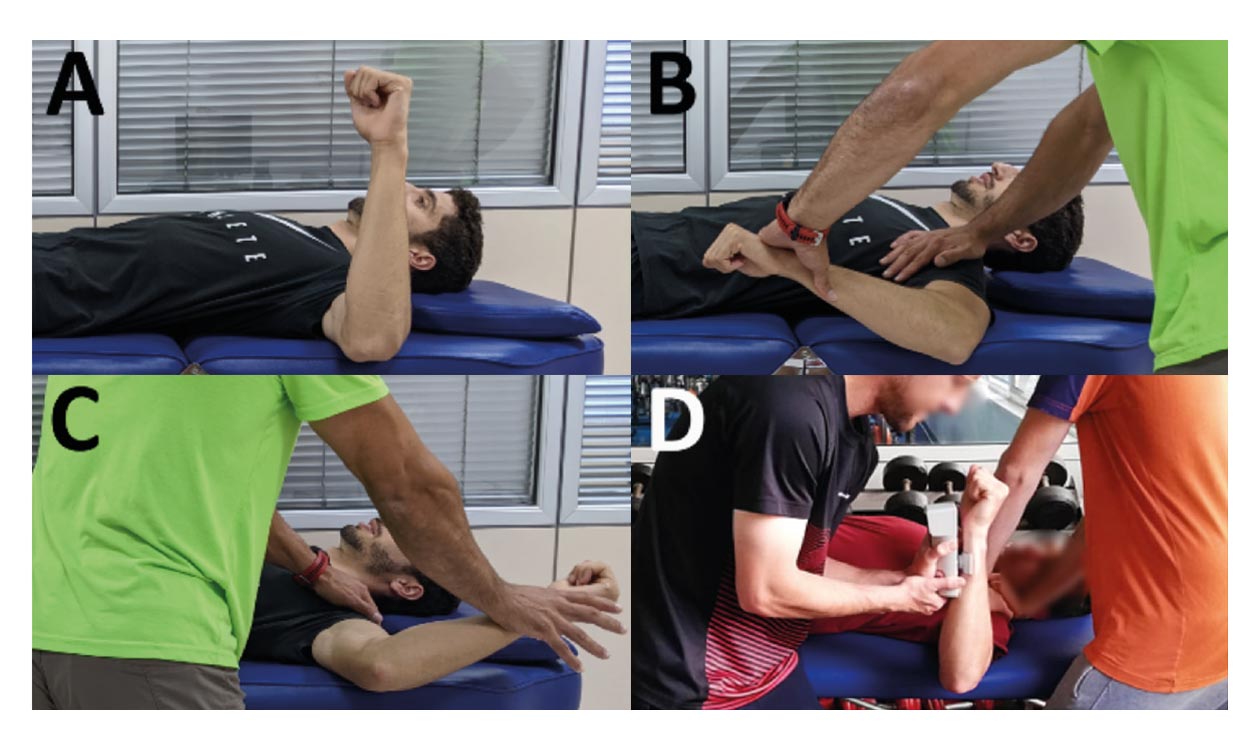
The aim of this test was to measure the shoulder joint ROM-IR and ROM-ER. For the execution of the test, participants were stretched out on a stretcher in the supine decubitus position, with the shoulder positioned at 90° of abduction, the elbow at 90° of flexion and in a neutral position of rotation (forearm perpendicular to the stretcher) (Moreno-Pérez et al., 2015) (Figure 1-A). The forearm was required to protrude laterally from the stretcher to allow maximum ROM-IR and ROM-ER of the scapulohumeral joint to be performed. This position was used as it is the position that bears the most similarities to the service movement for the execution of the ROM tests (Kibler et al., 1996). During the execution of the test, an investigator slowly pushed the distal part of the participant’s forearm until reaching the maximum ROM of IR or ER (Figure 1-B, Figure 1-C). With the other hand, the same researcher held the participant’s shoulder to avoid possible compensatory movements of the scapulothoracic region. The point of maximum rotation was considered to be the point at which the participant verbally expressed that he/she could not endure the passive movement any longer. Two attempts of the test were carried out for each arm and direction of rotation (IR and ER). Each attempt was recorded using a digital video camera (Casio Exilim High Speed EX-FH25) placed at stretcher height, perpendicular to the plane of movement, 5 metres away from the participant. The filming frequency of the camera was set to 60 Hz.
Peak isometric strength assessment test
The aim of this test was to assess the peak voluntary isometric strength (S) in the IR and ER movements of the scapulohumeral joint. A hand-held dynamometer (Nicholas Manual Muscle Tester by Lafayette Instrument Company, Model 01160) was used to obtain shoulder S-IR and S-ER, which provided strength values in kilograms (kg). For this test, participants were placed on a stretcher in the same starting position as described above for the ROM assessment test (Figure 1-D). The starting position ensured that the effects of gravity were removed and the muscles tested were placed in the middle of their range of motion (Amundsen, 1990). Two researchers were required to carry out this test. One researcher held the participant’s shoulder to avoid possible offsets. The other investigator positioned the hand-held dynamometer 2cm medial to the ulnar styloid process on the dorsal side of the participant’s forearm to measure S-ER and in the same location on the ventral side to measure S-IR. The dynamometer was held to prevent any movement of the participant’s arm (i. e., preventing IR or ER movement) (Cools et al., 2014, 2016; Riemann et al., 2010). Two attempts of the test were carried out for each arm and direction of rotation (IR and ER). For each attempt, the participant was encouraged to exert peak voluntary isometric IR or ER strength against the dynamometer for a time of 5 seconds (Amundsen, 1990). Participants were asked to progressively perform peak voluntary isometric strength and were allowed a 30-second rest between attempts. At the end of each attempt, the peak isometric strength value (kg) reached was recorded.
Data processing
ROM-IR and ROM-ER angles were obtained from footage processing during the ROM assessment test using Kinovea v0.8.15 (Puig-Diví et al., 2019). The ROM of each attempt was considered to be the absolute angle formed between the linear vector perpendicular to the stretcher and the vector between the anatomical points of the styloid process (mobile point) and the olecranon (fixed point). The ROM-T was calculated as the sum of the ROM-IR and ROM-ER angles (Gillet et al., 2017). For each arm, the average value of each variable was calculated with the values obtained from the two attempts (Couppé et al., 2012; Gillet et al., 2017; Moreno-Pérez et al., 2015).
In relation to the data from the peak isometric strength assessment test, the peak strength values recorded in each attempt were defined as S-IR and S-ER. All strength values were converted to newtons (N). For each arm, the average value of each variable was then calculated from the values obtained in the two test attempts (Couppé et al., 2012). Finally, from these mean values, the S-ER/S-IR ratio was calculated for each arm (Cools et al., 2016; Riemann et al., 2010).
Statistical Analysis
The data was tested for normal distribution using the Shapiro-Wilk normality test. Range of motion values (ROM-IR, ROM-ER and ROM-T) of the dominant arm (DA) and non-dominant arm (NDA) were compared using a paired samples Student’s t-test. In addition, the peak isometric strength variables (S-IR, S-ER and S-ER/S-IR) of both arms were also compared through a paired samples T-test. Statistical significance was set at p ≤ .050 for all analyses. The effect size of the different tests was expressed with Cohen’s d (1988) and with the following interpretation: 0.2 to 0.5, small effect; 0.5 to 0.8, medium effect; and more than 0.8, large effect.
Results
In relation to the first objective of the study, a comparison of the range of motion (ROM) of internal rotation (IR) and external rotation (ER) of the two arms (dominant: DA and non-dominant: NDA) was carried out (Table 1). The results of the paired samples T-test revealed significant differences between the DA and the NDA in terms of ROM-IR, with the NDA exhibiting a greater range of motion compared to the DA (23.73%) (Figure 2). Significantly higher ROM-T values were also observed in the case of the NDA (8.32%). No significant differences were observed in the ROM-ER comparison, indicating similar ROM between the two arms.
Table 1
Descriptive statistics of range of motion and peak isometric strength and results of bilateral comparison by paired samples T-test.

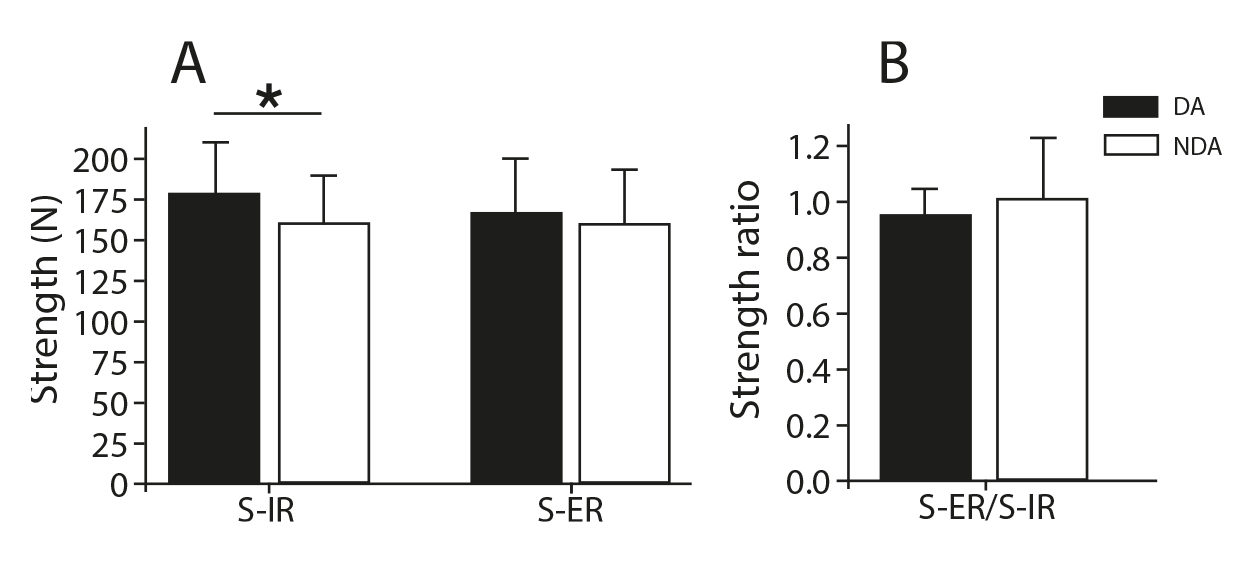
With regard to the second objective, a comparison of the peak isometric strength of both arms was carried out (Table 1). T-test results revealed a significantly higher S-IR of DA compared to NDA (9.67%) (Figure 3). No significant differences were found for the other variables of peak isometric strength.
Discussion
In tennis, the shoulder is one of the areas with the highest incidence of overuse injury. These injuries could be related to alterations in the range of motion and strength of the internal (IR) and external (ER) rotator muscles of the joint (Renstrom & Johnson, 1985). The aim of this study was to evaluate possible alterations in range of motion (ROM) and peak isometric strength (S) in the IR and ER movements of the shoulders in adult amateur tennis players. In order to achieve these objectives, a comparison of the racket grip arm or dominant arm (DA) and the non-dominant arm (NDA) was carried out.
In relation to ROM, DA was found to have a lower ROM-IR and ROM-T compared to NDA. In contrast, no differences were observed in ROM-ER, which could indicate that the differences found in ROM-T derive mainly from a reduction in ROM-IR. This is in line with other studies that also reported reductions in ROM-IR and ROM-T (Ellenbecker, 1992; Ellenbecker et al., 1996; Pluim et al., 2006). The lower ROM-IR found in the present study could be a reflection of the relatively advanced age and years of sport practice of the participants (Kibler et al., 1996; Moreno-Pérez et al., 2015). In contrast, in the present study a similar ROM-ER was observed between the two limbs. This result contrasts with previous studies, which revealed a higher ROM-ER in the DA of high-level players of different ages (Ellenbecker et al., 1996; Kibler et al., 1996; Moreno-Pérez et al., 2015). It is believed that increasing ROM-ER may enhance performance in overhead smashing or throwing actions by increasing the angular travel of these skills, thereby extending the acceleration time of the limb and thus facilitating the achievement of higher velocities at the end of the smash or throw (Hams et al., 2019). The fact that it is an adaption linked to the performance of the hitting gesture and the lack of differences in adult amateur athletes could imply that adaptations in ROM-ER are specific to high-level players.
These findings concerning the ROM could be relevant for the prevention of injuries in amateur tennis players. Range of motion differences between DA and NDA are often characterised as possible indicators of risk for shoulder joint injury (Pluim et al., 2006). Although there is no consensus on normative values for ROM in tennis players, an asymmetry between DA and NDA of less than 18° for ROM-IR and no more than 5° for ROM-T seems desirable (Cools et al., 2015; Wilk et al., 2011). Taking these values as a reference, the profile of the amateur player characterised in the present study could present a certain risk of shoulder injury given that bilateral differences in the ROM-IR (23.74%) and ROM-T (8.32%) are higher than the thresholds considered safe. In spite of this situation, the fact that a prerequisite for participation in this study was the absence of discomfort or injury to the shoulder joint limits the possibility of establishing a relationship between ROM disturbances and injury. Furthermore, the lack of agreed normative values for ROM in both healthy and injured tennis players limits the interpretation of the results of the present study. More studies are needed to explore the relationship between ROM disorders and shoulder joint injury in tennis, especially in amateur tennis players.
In the comparison of peak isometric strength values, higher S-IR values were observed for the DA compared to the NDA. These results are consistent with the results presented in the review by Pluim et al. (2006) where, in most of the studies analysed, tennis players had higher S-IR in the DA versus the NDA. On the other hand, in the present study, no differences were observed in either the S-ER or the S-ER/S-IR ratio between the DA and the NDA. Although the results indicated that there was a difference between arms in terms of S-IR, all other strength parameters exhibited similar values between limbs. Pluim et al. (2006) reported that higher S-IR values in the DA also contributed to a reduction in the S-ER/S-IR ratio values. Furthermore, this situation has been linked to the occurrence of shoulder joint pain and has been associated with the likelihood of injury (Gillet et al., 2018; Hams et al., 2019). Thus, despite the increase in S-IR in the DA, the absence of differences in S-ER and in the S-ER/S-IR ratio suggests that the participants in the present study may be relatively safe from potential shoulder injury with respect to strength-related risk factors. For example, the tennis players in this study would fall within the recommended range of the S-ER/S-IR ratio (between 0.75 and 1) proposed in previous publications (Cools et al., 2016). The absence of differences in the S-ER/S-IR ratio in the present study compared to previous publications (Pluim et al., 2006) could be explained by the absence of differences in S-ER and a lower difference in S-IR between arms. Therefore, it could be suggested that, similar to what has happened in the case of ROM-ER, the differences in S-ER and S-ER/S-IR ratio could be specific to high-level players, with training regimes of higher load (volume and intensity of play/training) than amateur players. Further studies are needed to determine the vulnerability of the amateur tennis player profile in relation to shoulder joint strength. The use of larger sample sizes, other peak strength assessment conditions (e.g., eccentric or concentric), and the inclusion of participants with a history of joint injury and/or discomfort may help to deepen understanding of this population.
Conclusions
In the present study of adult and amateur tennis players, less range of motion in internal rotation and total range of motion was observed in the dominant arm compared to the non-dominant arm. Also, greater peak isometric internal rotational strength was observed in the dominant arm compared to the non-dominant arm. These results, especially in relation to range of motion, suggest that adult amateur tennis players may be predisposed to shoulder injury in the dominant arm.
References
[1] Abrams, G., Renstrom, P., & Safran, M. (2012). Epidemiology of musculoskeletal injury in the tennis player. British Journal of Sports Medicine, 46, 492-498. https://doi.org/10.1136/bjsports-2012-091164
[2] Amundsen, L. (1990). Muscle Strength Testing. Instrument and Non-instrumented Systems. Chicago: Churchill Livingstone Inc.
[3] Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Mahwah, NJ: Lawrence Erlbaum Associates.
[4] Cools, A., De Wilde, L., Van Tongel, A., Ceyssens, C., Ryckewaert, R., & Cambier, D. (2014). Measuring shoulder external and internal rotation strength and range of motion: Comprehensive intra-rater and inter-rater reliability study of several testing protocols. Journal of Shoulder and Elbow Surgery, 23(10), 1454-1461. https://doi.org/10.1016/j.jse.2014.01.006
[5] Cools, A., Johansson, F., Borms, D., & Maenhout, A. (2015). Prevention of shoulder injuries in overhead athletes: A science-based approach. Brazilian Journal of Physical Therapy, 19(5), 331-339. https://doi.org/10.1590/bjpt-rbf.2014.0109
[6] Cools, A., Vanderstukken, F., Vereecken, F., Duprez, M., Heyman, K., Goethals, N., & Johansson, F. (2016). Eccentric and isometric shoulder rotator cuff strength testing using a hand-held dynamometer: reference values for overhead athletes. Knee Surgery, Sports Traumatology, Arthroscopy, 24(12), 3838-3847. https://doi.org/10.1007/s00167-015-3755-9
[7] Corbi, F., & Baiget, E. (2015). Differences in Isometric Strength Between the Dominant and Non-Dominant Upper Extremity in Competitive Tennis Players. Sport Science, 5(5), 19-21.
[8] Couppé, C., Thorborg, K., Hansen, M., Fahlström, M., Bjordal, J. M., Nielsen, D., Baun, M., Storgaard, M., & Magnusson, S. P. (2012). Shoulder rotational profiles in young healthy elite female and male badminton players. Scandinavian Journal of Medicine and Science in Sports, 24(1), 122-128. https://doi.org/10.1111/j.1600-0838.2012.01480.x
[9] Ellenbecker, T. (1992). Shoulder internal and external rotation strength and range of motion of highly skilled junior tennis players. Isokinetics and Exercise Science, 2(2), 65-72. https://doi.org/10.3233/IES-1992-2205
[10] Ellenbecker, T., Roetert, E., Piorkowski, P., & Schulz, D. (1996). Glenohumeral joint internal and external rotation range of motion in elite junior tennis players. Journal of Orthopaedic and Sports Physical Therapy, 24(6), 336-341. https://doi.org/10.2519/jospt.1996.24.6.336
[11] Felstead, A. J., & Ricketts, D. (2017). Biomechanics of the shoulder and elbow. Orthopaedics and Trauma, 31(5), 300-305. https://doi.org/10.1016/j.mporth.2017.07.004
[12] Gillet, B., Begon, M., Diger, M., Berger-Vachon, C., & Rogowski, I. (2018). Shoulder range of motion and strength in young competitive tennis players with and without history of shoulder problems. Physical Therapy in Sport, 31, 22-28. https://doi.org/10.1016/j.ptsp.2018.01.005
[13] Gillet, B., Begon, M., Sevrez, V., Berger-Vachon, C., & Rogowski, I. (2017). Adaptive alterations in shoulder range of motion and strength in young tennis players. Journal of Athletic Training, 52(1), 137-144. https://doi.org/10.4085/1062-6050.52.1.10
[14] Hams, A., Evans, K., Adams, R., Waddington, G., & Witchalls, J. (2019). Reduced shoulder strength and change in range of motion are risk factors for shoulder injury in water polo players. Physical Therapy in Sport. https://doi.org/10.1016/j.ptsp.2019.10.003
[15] Johnson, C., & McHugh, M. (2006). Performance demands of professional male tennis players. British Journal of Sports Medicine, 40, 696-699. https://doi.org/10.1136/bjsm.2005.021253
[16] Kibler, W., Chandler, T., Livingston, B., & Roetert, E. (1996). Shoulder Range of Motion in Elite Tennis Players. The American Journal of Sports Medicine, 24(3), 279-285. https://doi.org/10.1177/036354659602400306
[17] Kovacs, M. (2007). Tennis physiology: Training the competitive athlete. Sports Medicine, 37(3), 189-198. https://doi.org/10.2165/00007256-200737030-00001
[18] Moreno-Pérez, V., Moreside, J., Barbado, D., & Vera-Garcia, F. (2015). Comparison of shoulder rotation range of motion in professional tennis players with and without history of shoulder pain. Manual Therapy, 20, 313-318. https://doi.org/10.1016/j.math.2014.10.008
[19] Pluim, B., Staal, J., Windler, G., & Jayanthi, N. (2006). Tennis injuries: Occurrence, aetiology, and prevention. British Journal of Sports Medicine, 40, 415-423. https://doi.org/10.1136/bjsm.2005.023184
[20] Prieto-González, P., & Brahim, M. Ben. (2018). Treatment of shoulder impingement syndrome in adolescent tennis players. Apunts Educación Física y Deportes, 132, 32-47. https://doi.org/10.5672/apunts.2014-0983.es.(2018/2).132.03
[21] Prieto-González, P., & Larumbe-Zabala, E. (2021). ATR versus Traditional Periodization in Adolescent Amateur Tennis Players. Apunts Educación Física y Deportes, 144, 65-74. https://doi.org/10.5672/apunts.2014-0983.es.(2021/2).144.08
[22] Puig-Diví, A., Escalona-Marfil, C., Padullés-Riu, J. M., Busquets, A., Padullés-Chando, X., & Marcos-Ruiz, D. (2019). Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE, 14(6), 1-14. https://doi.org/10.1371/journal.pone.0216448
[23] Real Federación Española de Tenis. (2021). Memoria 2021.
[24] Renstrom, P., & Johnson, R. (1985). Overuse Injuries in Sports. Sports Medicine. Sport Medicine, 2, 316-333. https://doi.org/10.2165/00007256-198502050-00002
[25] Riemann, B., Davies, G., Ludwig, L., & Gardenhour, H. (2010). Hand-held dynamometer testing of the internal and external rotator musculature based on selected positions to establish normative data and unilateral ratios. Journal of Shoulder and Elbow Surgery, 19, 1175-1183. https://doi.org/10.1016/j.jse.2010.05.021
[26] Van Der Hoeven, H., & Kibler, W. (2006). Shoulder injuries in tennis players. British Journal of Sports Medicine, 40, 435-440. https://doi.org/10.1136/bjsm.2005.023218
[27] Wilk, K., MacRina, L., Fleisig, G., Porterfield, R., Simpson, C., Harker, P., Paparesta, N., & Andrews, J. (2011). Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. American Journal of Sports Medicine, 39(2), 329-335. https://doi.org/10.1177/0363546510384223
ISSN: 2014-0983
Received: November 3, 2022
Accepted: February 22, 2023
Published: October 1, 2023
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


