Relationship between Strength and Self-Perception of Independence in Activities of Daily Living of Paraplegic Adults
Carlos Val-Serrano

Saleky García-Gómez
*Corresponding author: Carlos Val-Serrano carlos_val_86@hotmail.com
Cite this article
Val-Serrano, C., & García-Gómez, S. (2020). Relationship between Strength and Self-Perception of Independence in Activities of Daily Living of Paraplegic Adults. Apunts. Educación Física y Deportes, 142, 1-7. https://doi.org/10.5672/apunts.2014-0983.es.(2020/4).142.01
Abstract
The objective of this study was to examine whether there was a relationship between relative strength development and self-perception of independence in adults with paraplegia six weeks after a physical activity intervention. For this purpose, a sample of eight people with paraplegia was evaluated, five men and three women, with a mean age of 29.5 ± 5.17 years, with spinal cord injury below D5, and who had not performed physical activity previously. The relative strength index was used to measure body capacity together with the Barthel index questionnaire to evaluate independence in activities of daily living. The results showed a very high significant Pearson’s correlation coefficient between changes in relative strength and the questionnaire (.93), as well as an 87.1 % coefficient of determination. The mean percentage increase in the participants’ relative strength was 25.52 %, accompanied by a 16.54 % increase in the questionnaire score. In conclusion, there was a direct relationship between relative strength and the self-perception of adults with paraplegia of their independence in daily life, which shows that an intervention programme leads to significant changes in relative strength and self-perception of independence.
Introduction
In general terms there are various benefits of engaging in physical activity for people with disabilities (Gallego et al., 2016), such as improved self-concept and independence. These benefits are also observed in paraplegia (Kawanishi & Greguol, 2013) and these factors are essential for devising social inclusion strategies for people with physical disabilities (Macías García & González López, 2012). Accordingly, this study contends that adapted physical activity has been conceived as a means of rehabilitation, and there are several studies which examine features related to performance (Castelli Correia de Campos et al., 2019) and quality of life.
Some papers report that upper body strength is crucial in the activities of daily living of people with paraplegia (Gottlob, 2008), although there are almost no studies about the impact of relative strength on the self-perception of independence in activities of daily living of people with paraplegia.
There is little scientific evidence relating relative strength and the perception of independence. In this respect, relative strength means the ability to lift and accelerate body movement (National Strength and Conditioning Association, NSCA). Similarly, Barrero, García-Arrioja and Ojeda (2005) define self-perception of independence as a person’s own assessment of their functional capacity in their activities of daily living.
A previous study (Jiménez, Martín, Abadía, & Herrero, 2007) presents similarities with the purpose of this paper by establishing the influence of strength endurance on physical condition in individuals with spinal cord injuries in wheelchairs between the ages of 22 and 39, where strength is a basic physical ability which, in addition to the biological domain, may also affect other areas of people’s lives (Kawanishi & Greguol, 2013). In all these cases, strength is said to be related to physical self-concept.
In terms of independence, Penninx et al. (2001) describe a study comparing the development of strength with independence and the prevention of acquired disability. However, in their conclusions they argue that endurance, rather than strength, is the basic physical capacity which can grant independence and prevent disability. There are also studies (Martins, Alberto, & Massoli, 2019) that show the impact of ergonomics on the performance of an activity in people with physical disabilities.
As for the potential impact of strength endurance on relative strength, Jiménez et al. (2007) hold that strength endurance cannot alter maximal strength and therefore cannot alter relative strength either. A distinction is drawn between maximal strength and relative strength, whereby the latter is determined by dividing the kilos lifted at maximal strength by the kilos of the individual’s body weight (Bompa, 2003). It is germane to underline this, since the programme to be used in this study would not see changes in either maximal or relative strength. Thus, the relationship between psychological and social factors is significant when the impact of this basic physical capacity on aspects of wellbeing and functionality (Serra, 2011) is considered. However, hitherto, relative strength has not been shown to be related to self-perception of independence.
Moreover, since previous studies did not clarify whether exercises focused on developing basic physical abilities such as strength, endurance, speed and flexibility might have positive effects on wheelchair users, other training methods or systems need to be brought into play. According to on this premise, there is a controversy in which it is suggested that “the progress of maximal strength does not correspond to an equal increase in strength endurance or speed strength, since a successive reduction in these specific abilities immediately becomes apparent if the training is not modified” (Mirella, 2001, p. 54), which indicates whether training focused on developing strength endurance may influence relative strength. Similarly, the relationship between the results of tests in which one muscle group is primarily involved and those obtained by evaluating the muscle activity of the opposite muscle group is unknown. Furthermore, in the general population, the relationship between the development of strength and the subjective perception of factors other than physical self-concept is unknown, bearing in mind that other feelings which influence the individual and collective development of each person must also be taken into account. Moreover, neither are the perceptions of people with paraplegia of their independence and its possible relationship with basic physical abilities known.
The objective of this study was to examine whether there was a relationship between relative strength development and self-perception of independence in adults with paraplegia by measuring relative strength using the shoulder muscle group, exploring whether this was related to self-perception of independence in the activities of daily living of adults with paraplegia. Furthermore, the degree of such an influence was examined and the mean percentage of variation in both relative strength and self-perception of independence after a six-week intervention programme was obtained. There are also the particularities of focusing on the development of a type of strength opposite to relative strength, namely strength endurance (Bompa, 2003; Jimenez et al., 2007). Therefore, the study was also designed to observe the development of relative strength in the shoulder muscle group, which is antagonistic to the dorsal muscle group (Willmore & Costill, 2004), the main group in the activities of daily living of people with paraplegia (Gottlob, 2008).
Methodology
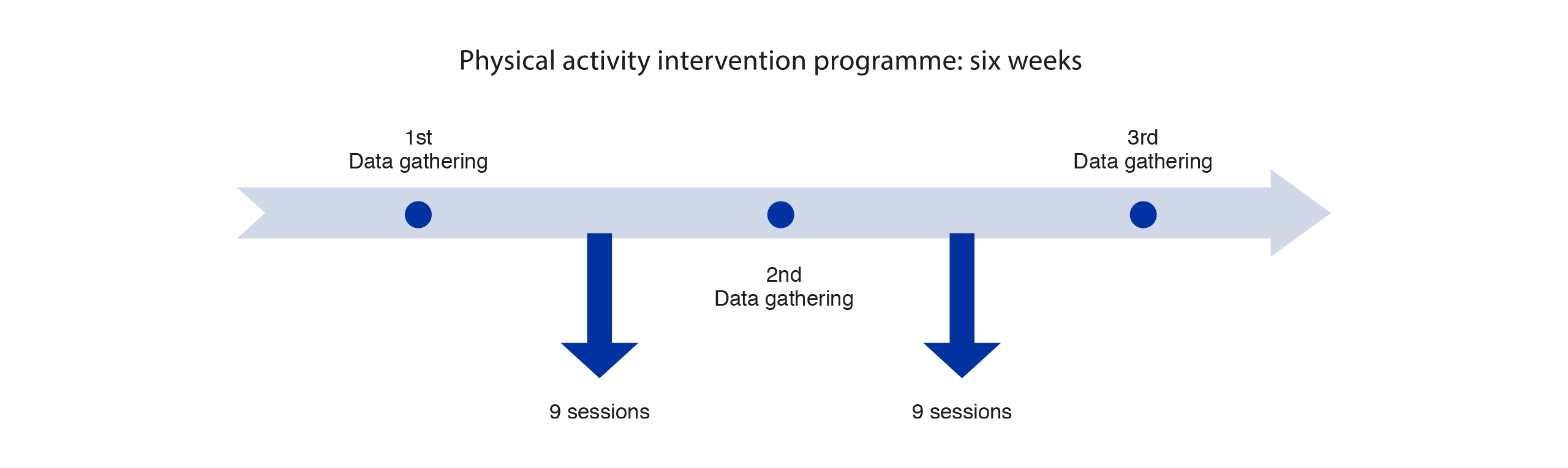
A quasi-experimental longitudinal follow-up study was performed with a pre-post facto design based on a six-week intervention. The physical activity programme involved working on the strength endurance of the upper body muscles, specifically the pectoral, dorsal, abdominal, biceps and triceps. The exercises were based on calisthenics and free weights mainly with dumbbells, following the structure of four series of 20 repetitions each with 40 seconds’ rest between each series, as in the study carried out by Willmore and Costill (2004).
Figure 1 shows the design of the study derived from the objective.
Participants
The sample was comprised of eight people with physical-motor disabilities, five men and three women, with an age range between 22 and 39 years (29.5 ± 5.17) and residing in the Community of Madrid. The inclusion criteria specified: a) having a spinal cord injury; b) having a spinal cord injury below D5; c) having an ASIA C, D or E scale (American Spinal Injury Association, ASIA); d) not performing any kind of physical or sports activity in their daily lives prior to the study; and e) not undergoing continuous weight changes prior to the study. The exclusion criteria were as follows: not having physical-motor disability combined with another form of disability and not performing intense physical activity in their jobs.
All the participants were informed about all the activities to be carried out in the study before it and signed the informed consent form to indicate their voluntary participation and commitment. The study protocol was approved by the Autonomous University of Madrid Ethics Committee and also complied with the guidelines of the Declaration of Helsinki (2000).
Instruments
Barthel Index questionnaire
The Barthel Index questionnaire (Granger et al., 1979) was used to evaluate independence in the activities of daily living of people with disabilities. The questionnaire consisted of 10 items assessed using a Likert scale, each one with a score of 0 to 4. It was tailored to the needs of the study, as it is a questionnaire which can be adapted, and both the number of items and the score can be chosen, according to Barrero, García-Arrioja and Ojeda (2005).
The items specified in the questionnaire were: Personal hygiene, Getting in and out of the shower, Eating, Using the toilet, Going up and down stairs, Getting dressed, Moving from wheelchair to bed and returning, Moving without wheelchair, Moving with wheelchair, Getting in and out of wheelchair. The scores meant: unable to do so (0); tries to do so but is insecure (1); some assistance needed (2); minimal assistance needed (3); and totally independent (4). The range of scores was therefore from 0 to 40 points. The higher the score, the more independent the participants felt. Conversely, the lower the score, the less independent they felt.
Relative strength
The NSCA defines relative strength as the ability to lift and accelerate body movement, giving the result of maximal strength (Smax=1 RM) divided by body weight (BW).
Procedure
Firstly, the participants were informed about the process and then completed the Barthel Index questionnaire (BIQ) based on the points explained.
Body weight was then measured; the participants were weighed using a scale with a margin of error of one gram per kilogram of weight measured, and the data were also recorded to the first decimal place (kilos and hectograms). The measurement taken made in the same time interval for each participant, who wore the same clothing for all measurements, consisting of underwear, socks, trousers and T-shirt. In order to ensure that measurements were taken in the same conditions, all the participants were weighed at a set time after their last food intake, as this is an influential factor (Casanueva et al., 2008). This datum was gathered on two consecutive occasions and was considered valid when the scales showed the same weight both times.
Subsequently, the front shoulder press exercise was performed to measure maximal strength using a 4.5-kilo bar and discs of varying weight. In the exercise, participants performed 10 repetitions with the maximum weight they felt they could manage, calculating maximal strength at 70% of this amount (Cronin & Hansen, 2005). The 10-repetition procedure was used instead of a maximum repetition in order to reduce the risk of injury to participants, since higher loads increased such risk (Willmore & Costill, 2004).
Exercise performance consisted of vertical movement of the arms from a position in which they were parallel to the ground (90-degree elbow flexion) to maximum extension above the head (total elbow extension). The participants sat on a chair used by all of them, to which their trunk was securely fixed by means of Velcro straps in order to avoid compensation by other muscles not required in the exercise (Monroy, 2011). A stopwatch was also employed to set the exact same rest time between possible repetitions of the exercise by some participants, as they sometimes performed the exercise and at the end of it felt they could lift more weight. A three-minute rest time was set, which was appropriate for achieving maximum efficacy in the maximal strength method (Bompa, 2003). Finally, these data were used to record the relative strength index, the result of dividing the kilos of maximal weight lifted by the kilos of body weight of each one of the participants, which was noted on a datasheet.
After the measurements, the participants began the physical activity programme, which consisted of exercises designed to develop strength, endurance, speed and flexibility (Mirella, 2006).
The intervention was organised into nine one-hour sessions held three times a week. After three weeks, the variables were measured. On the following day, the second part of the programme was resumed, consisting of the remaining nine sessions. Finally, after six weeks the variables were measured for the third and last time. Three measurements were chosen to verify whether the changes occurring between the first and third measurements followed a consistent order during the middle stage of the experimental process (Arnau & Bono, 2008).
Data analysis
The data were recorded using Microsoft Excel 2010 Professional Plus, and the statistical analysis was performed using SPSS version 22. The data met a normal distribution according to the Shapiro-Wilk test (Pedrosa et al., 2015). As the study was longitudinal, the general linear model (Arnau & Bono, 2008) was used to analyse repeated measurements with a significance level of p < .05 to check for significant differences in changes in relative strength and BIQ score during the process, and the Bonferroni interval adjustment was added to compare the three pre-, intermediate and post- study measures in pairs (Gil, 2015). In addition, the Pearson correlation coefficient was applied to extract the type of relationship in the changes produced between both variables (Pedrosa et al., 2015). In the interpretation of this type of relationship, values of < .20 were considered as very low; between .20 and .39 as low; between .40 and .59 as moderate; between .60 and .79 as high; and between .80 and 1 as very high (Morrow et al., 2005). Similarly, the coefficient of determination was extracted to obtain the percentage of reliability that the potential changes in relative strength would impact the change in the Barthel Index questionnaire score (Pedrosa et al., 2015). Meanwhile, the percentages of each participant were calculated and then added up and the total was divided by the study sample to establish the mean variation percentages.
Table 1
Evolution of relative strength and BIQ between the first and last measurements.
Results
As can be seen in Table 1, the study participants presented changes in both their relative strength and BIQ. In relative strength, positive changes were observed, except in participants 4 and 6. Furthermore, positive changes in BIQ were seen after the intervention.
The operability of relative strength comprised an unlimited range, while in BIQ the response range was between 0 and 40. Finally, table 2 shows that there were significant changes in both study variables, with greater variation in relative strength than in BIQ scores.
Table 2
Descriptive values.
The results indicated a direct correlation between relative strength and BIQ scores (r = .933), which was considered very high, showing that changes in relative strength in each one of the participants were related to BIQ scores across all three data measurements in the study. Thus, the coefficient of determination presented a high-influence value (R² = .871), which meant that there was an 87.1% probability that the variation in the BIQ score over the three measurements could be explained by the changes in relative strength.
Discussion
This paper focused on the impact of relative strength on self-perception of independence in the activities of daily living of adults with paraplegia. It also explored the degree of relative strength, and additionally determined the mean percentage of variation in relative strength and self-perception of independence separately.
The most significant result of the study was the assertion that changes in relative strength are strongly associated with this population’s self-perception of independence. Furthermore, the percentage increase in the group mean for relative strength represented a substantial improvement.
Unlike previous research (Serra, 2011), this paper showed variations in relation to relative strength. The results point to significant changes in relative strength after six weeks of intervention in people with paraplegia; however, there are studies in people with intellectual disability whose performance is lower after doing strength tests (Cabeza Ruiz & Castro Lemus, 2017), whereby a certain degree of caution is required when generalising the findings. In this respect, the proposed intervention may bring about significant changes in adults with paraplegia who do not perform any other physical activity outside the programme or any other physical activity prior to it.
Taking previous studies as a reference, Jiménez et al. (2007) studied the implications of strength endurance for speed and fatigue, it being considered that the development of relative strength has proportional changes together with these two factors in the independence of adults with paraplegia. Strength endurance was worked on in the physical activity programme analysed and led to positive changes in relative strength. However, studies by other researchers found no impact at all. Mirella (2001) does not draw precise conclusions about the influence of relative strength on independence, which is why these results differ from previous studies.
It is important to stress that the literature concerning relative strength in people with physical disabilities is scant, which constitutes a challenge in conducting research in this group. While there are a number of studies in which strength measurements were taken in wheelchair users (Wilbanks & Bickel, 2016; Cabeza Ruiz & Castro Lemus, 2017), these studies did not address relative strength.
In terms of the characteristics of the physical activity programme, this paper is similar to that of Hicks et al. (2003), who observe no significant changes in the first stage of their programme, hence self-perception and external perception might be said to present discrepancies with regard to independence taking the intervention into account.
Similarly, Hicks et al. (2003) established a nine-month physical activity programme with two weekly sessions to observe the possible transference from strength development to independence. By contrast, in this study, changes were apparent after three weeks, bearing in mind that in both sets of research none of the participants had done any previous physical activity.
With regard to the recording of relative strength data, resources such as MuscleLab are recommended as a reliable tool for ascertaining maximal strength, since Padullés and López (2011) argue that it can identify and describe the events which occur in muscle contraction. This would make it possible to confirm, with the utmost confidence, that each participant used their muscle fibres involved in the effort at the maximum possible contraction.
There were two specific limitations with regard to body weight. The first was weight variation throughout the process. Although these weight changes were minor and the differences were not significant (.231>.05), the participants’ weight fluctuations ranged from a .6 kg gain to a 1.6 kg loss. The second limitation was in the intake times prior to weighing on the scale.
Adherence to the programme was 72.7%. This figure reflects the number of participants who completed the full physical activity programme, since three participants dropped out of the study for personal reasons; these withdrawals do not influence the results, because in these cases only the first data set had been collected. In this respect, it would be useful to explore this question in greater depth in a larger sample in future research designed to compare the different types of strength and ascertain which one would have the greatest impact on factors such as independence or self-perception of independence in people with paraplegia, as well as in studies focusing on self-perception in this population group.
Conclusion
After six weeks of intervention there were significant changes in terms of relative strength and self-perception of independence which improve the performance of activities of daily living. Using the BIQ and measuring relative strength are recommended as tools for supervising and monitoring a physical activity and strength programme in people with paraplegia for initiation and also to establish functional changes during the rehabilitation and recovery process. In this respect, it is important to underscore the need to set clear targets when implementing an intervention, include strength and endurance exercises in programmes targeting wheelchair users, and also to factor in self-perception of independence in order to enhance their quality of life.
Acknowledgements
The authors would like to thank the participants and the ASPIMIP institution for their cooperation in carrying out this study.
References
[1] Arnau, J.,& Bono, R. (2008). Estudios longitudinales de medidas repetidas. Modelos de diseño y análisis. Escritos de Psicología, 2(1), 32-41. ISSN: 1138-2635
[2] Barrero, C. L., García-Arrioja, S., & Ojeda, A. (2005). Índice de Barthel (IB): Un instrumento esencial para la evaluación funcional y la rehabilitación. Plasticidad y Restauración Neurológica, 4(1-2), 81-85.
[3] Bompa, T. O. (2003). Periodización. Teoría y metodología del entrenamiento. Barcelona: Hispano Europea.
[4] Cabeza Ruiz, R., & Castro Lemus, N. (2017). Hand Grip Strength in Adults with Intellectual Disabilities. Apunts. Educación Física y Deportes, 129, 44-50. https://doi.org/10.5672/apunts.2014-0983.es.(2017/3).129.03
[5] Casanueva, E., Kaufer, M., Pérez-Lizaur, A. B., & Arroyo, P. (2008). Nutriología médica. México: Panamericana. ISBN: 9786079356545
[6] Castelli Correia de Campos, L. F., Ribeiro da Luz, L. M., Luarte Rocha, C. E., Diehl Nogueira, C., Labrador Roca, V., & Irineu Gorla, J. (2019). Validation of Test Studies for the Analysis of Aerobic Power in Tetraplegic Athletes. Apunts. Educación Física y Deportes, 135, 68-81. https://doi.org/10.5672/apunts.2014-0983.es.(2019/1).135.05
[7] Cronin, J. B., & Hansen, K. T. (2005). Strength and power predictors of sports speed. The Journal of Strength & Conditioning Research, 19(2), 349-357 https://doi.org/10.1519/14323.1
[8] Gallego, J., Aguilar, J., Cangas, A. J., Pérez-Escobar, M. J.,& Barrera, S. (2016). Hábitos de actividad física en mujeres con discapacidad: relación con sus características físicas y funcionales. Revista Iberoamericana de Psicología del Ejercicio y el Deporte, 9(2), 471-494.
[9] Gil, J. A. (2015). Metodología cuantitativa en educación. Madrid: UNED. ISBN: 9788436261394
[10] Gottlob, A. (2008). Entrenamiento Muscular Diferenciado. Tronco y Columna Vertebral. Barcelona: Paidotribo. ISBN: 9788480199193
[11] Granger, C. V., Dewis, L. S., Peters, N. C., Sherwood, C. C., & Barrett, J. E. (1979). Stroke rehabilitation: analysis of repeated Barthel index measures. Archives of Physical Medicine and Rehabilitation, 60(1), 14-17.
[12] Thomas, J. R., Nelson, J. K., & Mata, M. J. (2007). Métodos de investigación en actividad física. Paidotribo.
[13] Hicks, A. L., Martin, K. A., Ditor, D. S., Latimer, A. E., Craven, C., Bugaresti, J., & McCartney, N. (2003). Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord, 41(1), 34-43. https://doi.org/10.1038/sj.sc.3101389
[14] Jiménez, B., Martín, J., Abadía, O., & Herrero, J. A. (2007). Entrenamiento de fuerza del miembro superior en usuarios de silla de ruedas. Revista Internacional de Medicina y Ciencias de la Actividad Física y el Deporte, 7(27), 232-240. ISSN: 1577-0354
[15] Kawanishi, C. Y., & Greguol, M. (2013). Physical activity, quality of life, and functional autonomy of adults with spinal cord injuries. Adapted Physical Activity Quarterly, 30(4), 317-337. https://doi.org/10.1123/apaq.30.4.317
[16] Macías García, D., & González López, I. (2012). Social Inclusion of People with Physical Disabilities through High Performance Swimming. Apunts. Educación Física y Deportes, 110, 26-35. https://doi. org/10.5672/apunts.2014-0983.es.(2012/4).110.03
[17] Martins, G., Alberto, L., & Massoli, G. (2019). Shot Put: Ergonomic Analysis in the Adapted Sport. Apunts. Educación Física y Deportes, 136, 113-128. https://doi.org/10.5672/apunts.2014-0983.es.(2019/2).136.08
[18] Mirella, R. (2001). Las nuevas metodologías del entrenamiento de la fuerza, la resistencia, la velocidad y la flexibilidad. Barcelona: Paidotribo. ISBN: 9788480195782
[19] Monroy, A. J. (2011). Guía práctica de musculación: el miembro superior. Sevilla: Wanceulen. ISBN-10: 8498236444
[20] Morrow, J. R., Jackson, A. W., Disch, J. G., & Mood, D. P. (2005). Measurement and Evaluation in Human Performance. Champaign: Human Kinetics. ISBN: 1450470432
[21] Padullés, J. M., & López, J. L. (2011). Valoración de la fuerza dinámica en la fase concéntrica del medio squat con atletas velocistas mediante la tecnología Ergo Power conectada al Musclelab. Colección ICD: Investigación en Ciencias del Deporte, 21.
[22] Pedrosa, I., Juarros, J., Robles, A., Basteiro, J., & García-Cueto, E. (2015). Pruebas de bondad de ajuste en distribuciones simétricas, ¿qué estadístico utilizar? Universitas Psychologica, 14(1), 245-254. https://doi.org/10.11144/Javeriana.upsy14-1.pbad
[23] Penninx, B. W., Messier, S. P., Rejeski, W. J., Williamson, J. D., Di Bari, M., Cavazzini, C., & Pahor, M. (2001). Physical exercise and the prevention of disability in activities of daily living in older persons with osteoarthritis. Arch Intern Med 2001, 161(19), 2309-2316. https://doi.org/10.1001/archinte.161.19.2309
[24] Serra, M. P. (2011). Determinación de los efectos del entrenamiento de fuerza de la cintura escapular en parapléjicos usuarios de silla de ruedas (Tesis doctoral). Universidad de Valencia, Valencia.
ISSN: 2014-0983
Received: 14 February 2020
Accepted: 25 May 2020
Published: 1 October 2020
Editor: © Generalitat de Catalunya Departament de la Presidència Institut Nacional d’Educació Física de Catalunya (INEFC)
© Copyright Generalitat de Catalunya (INEFC). This article is available from url https://www.revista-apunts.com/. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en


